clinical watse tesis
TRANSCRIPT

UNIVERSITI TEKNOLOGI MALAYSIA
BORANG PENGESAHAN STATUS TESIS ♦
JUDUL : CLINICAL WASTE MANAGEMENT AND DISPOSAL (CASE STUDY: HOSPITAL TENGKU AMPUAN RAHIMAH,
KLANG, SELANGOR)
SESI PENGAJIAN: 2006 / 2007
Saya, CHONG KIN FOOK (HURUF BESAR)
mengaku membenarkan tesis (PSM / Sarjana / Doktor Falsafah)* ini disimpan di Perpustakaan Universiti Teknologi Malaysia dengan syarat-syarat kegunaan seperti berikut: 1. Tesis adalah hakmilik Universiti Teknologi Malaysia. 2. Perpustakaan Universiti Teknologi Malaysia dibenarkan membuat salinan untuk tujuan
pengajian sahaja. 3. Perpustakaan dibenarkan membuat salinan tesis ini sebagai bahan pertukaran antara
institusi pengajian tinggi. 4. **Sila tandakan ( )
SULIT
(Mengandungi maklumat yang berdarjah keselamatan atau kepentingan Malaysia seperti yang termaktub di dalam AKTA RAHSIA RASMI 1972)
TERHAD
(Mengandungi maklumat TERHAD yang telah ditentukan oleh organisasi/badan di mana penyelidikan dijalankan)
√
TIDAK TERHAD
Disahkan oleh
(TANDATANGAN PENULIS) (TANDATANGAN PENYELIA) Alamat tetap
86, JLN BATU NILAM 8, BANDAR BUKIT TINGGI, EN. MOHD NOR OTHMAN 41200, KLANG, SELANGOR Nama Penyelia
Tarikh: 16 APRIL 2007 Tarikh: 16 APRIL 2007 CATATAN: * Potong yang tidak berkenaan. ** Jika tesis ini SULIT atau TERHAD, sila lampirkan surat daripada pihak berkuasa/ organisasi berkenaan dengan menyatakan sekali sebab dan tempoh tesis ini perlu dikelaskan sebagai SULIT atau TERHAD. Tesis dimaksudkan sebagai tesis bagi Ijazah Doktor Falsafah dan Sarjana secara penyelidikan, atau disertasi bagi pengajian secara kerja kursus dan penyelidikan, atau Laporan Projek Sarjana Muda (PSM)

“I hereby declare that I have read this thesis and in
my opinion this thesis is sufficient in terms of scope and
quality for the award of the degree of Engineering (Civil)”
Signature : ...................................................
Name of Supervisor : En Mohd Nor Othman
Date : 16 April 2007

CLINICAL WASTE MANAGEMENT AND DISPOSAL (CASE STUDY: HOSPITAL TENGKU AMPUAN RAHIMAH,
KLANG, SELANGOR)
CHONG KIN FOOK
A report submitted in partial fulfillment of the requirements for the award of the degree of
Bachelor of Engineering (Civil)
Faculty of Civil Engineering Universiti Teknologi Malaysia
APRIL 2007

PENGURUSAN DAN PELUPUSAN SISA KLINIKAL (KAJIAN KES: HOSPITAL TENGKU AMPUAN RAHIMAH,
KLANG, SELANGOR)
CHONG KIN FOOK
Laporan projek ini dikemukakan sebagai memenuhi sebahagian daripada syarat penganugerahan
Ijazah Sarjana Muda Kejuruteraan Awam
Fakulti Kejuruteraan Awam Universiti Teknologi Malaysia
APRIL 2007

ii
I declare that this thesis entitled “ Clinical Waste Management and Disposal (Case
Study: Hospital Tengku Ampuan Rahimah, Klang, Selangor “ is the result of my own
research except as cited in the references. The thesis has not been accepted for any
degree and is not concurrently submitted in candidature of any other degree.
Signature : ....................................................
Name : CHONG KIN FOOK
Date : 16 April 2007

iii
Specially dedicated to my family, my beloved parents and siblings
Thank you for the love and support
For my friends and coursemates (SAW 2002-2007)
Thank you for the memories and friendship

iv
ACKNOWLEDGEMENT
The successful completion would be impossible without the assistance and
guidance of many individuals who have provided invaluable help to me directly and
indirectly throughout my whole research. I would like to express my gratitude to
every individual who has contributed to this research.
I would like to thank my supervisor, En Mohd Nor Othman who has provided
guidance and advice to my research. His endless support and invaluable critics have
help me a lot in this research.
I would like to thank to all of the staffs in Hospital Tengku Ampuan Rahimah,
Klang who have cooperated with me during the research. Special thanks to Dr Enna
and Cik Norzilah from the quality unit who have contributed tremendously to my
research. I would also like to thank the staffs from Radicare (M) Sdn Bhd who have
provided a lot of assistance to my research.
Finally, I would like to thank my parents for their love and support. I would
like to thank my friends who have helped me directly or indirectly in the research.

v
ABSTRAK Pengurusan dan pelupusan sisa klinikal di Malaysia adalah menggunakan
prinsip “dari buaian ke kubur” dan di bawah kawalan Akta Kualiti Alam Sekitar
(Sisa Berjadual)1989. Penjana dan kontraktor dilantik adalah bertanggungjawab ke
atas pengurusan dan pelupusan sisa klinikal. Penjanaan sisa klinikal memerlukan
suatu pelan pengurusan terperinci supaya setiap komponen seperti pengasingan dan
pengangkutan bekerjasama antara satu sama lain. Pengurusan yang tidak rapi boleh
menyebabkan pendedahan kepada penyakit berbahaya seperti AIDS. Garis panduan
tertentu harus diikuti semasa mengurus sisa klinikal berbahaya seperti benda tajam.
Kos pelupusan sisa klinikal tinggi dan membawa risiko berbahaya yang berpunca
dari sisa perubatan serta menurunkan nilai estetik. Walaupun tiada kes serius seperti
kemalangan yang berkaitan dengan sisa klinikal dilapori sebelum ini, kesedaran staf
hospital dalam sistem pengurusan perlu di tahap tinggi pada setiap masa.

vi
ABSTRACT
Management and disposal of clinical waste in Malaysia using cradle-to-grave
concept is under the jurisdiction of Environmental Quality (Scheduled Waste)
Regulation 1989. The generator and the contractor appointed bear the sole
responsibilities in managing and disposing the clinical wastes. Generation of clinical
waste need a comprehensive management plan in order for each and every elements
such as segregation or transportation to work in tandem with each other. Poor
management of clinical waste can lead to high risk of exposure of dangerous diseases
such as AIDS. Certain guidelines are needed to handle special clinical wastes such as
sharps. Clinical wastes are costly in disposal and carry risks of infection, or physical
injury, and of exposure to potentially harmful pharmaceuticals, as well as being
aesthetically unacceptable. Though no serious case of accidents related to clinical
waste have ever been reported, awareness of the healthcare staffs in the management
system need to be at high level at all time.

vii
TABLE OF CONTENTS
CHAPTER TITLE PAGE
TITLE PAGE
DECLARATION ii
DEDICATION iii
ACKNOWLEDGEMENT iv
ABSTRAK v
ABSTRACT vi
TABLE OF CONTENTS vii
LIST OF TABLES x
LIST OF CHARTS xi
LIST OF FIGURES xii
LIST OF APPENDICES xiii
I INTRODUCTION
1.1 Background Study 1
1.2 Objectives 2
1.3 Problem Statement 2
1.4 Scope of Research 3
1.5 Significance of Study 3
1.6 Expected Results 4

viii
II LITERATURE REVIEW
2.1 Categories of Medical Waste 5
2.1.1 Human Blood and Blood Products 7
2.1.2 Cultures and stocks of infectious agents 8
2.1.3 Pathological wastes 9
2.1.4 Contaminated sharps 10
2.1.5 Contaminated laboratory wastes 12
2.1.6 Contaminated wastes from patient care 13
2.1.7 Discarded Biologicals 14
2.1.8 Contaminated animal carcasses, body parts
and bedding 15
2.1.9 Contaminated equipment 15
2.1.10 Miscellaneous infectious wastes 16
2.2 Medical waste management 16
2.2.1 Management plan 17
2.2.2 Identification 18
2.2.3 Segregation, containment, and labeling 18
2.2.4 Storage 20
2.2.5 Treatment 20
2.2.6 Transportation 20
2.2.7 Record Keeping 21
2.2.8 Staff Training 21
2.3 Clinical waste laws and regulations 22
III METHODOLOGY
3.1 Literature review 24
3.2 Site Visits 25
3.3 Interview 25
ix
3.4 Questionnaire 26
3.4.1 Gender 27
3.4.2 Age 27
3.4.3 Years of working 28
3.4.4 Scope of work 28
3.4.5 Scaled questions 28
IV RESULTS AND ANALYSIS
4.1 Introduction 30
4.2 Clinical waste management 30
4.2.1 Background of hospital 31
4.2.2 Processes of clinical waste management 34
4.2.2.1 Identification and segregation 34
4.2.2.2 Labelling and packaging 36
4.2.2.3 Internal transportation 39
4.2.2.4 Storage 39
4.2.2.5 External transportation 40
4.2.2.6 Incineration 42
4.3 Analysis of the survey 43
4.3.1 General questions analysis 43
4.3.2 Scaled questions analysis 47
V CONCLUSIONS AND RECOMMENDATIONS
5.1 Latest development of clinical waste generation 55
5.2 Conclusion 58
5.3 Recommendation 59
5.4 Further Studies 60
REFERENCES 61
APPENDICES 63-65

x
LIST OF TABLES
TABLE NO. TITLE PAGE 4.1 The distribution groups for segregating clinical wastes 35 4.2 Different colour codes for the purpose of packaging 36

xi
LIST OF FIGURES
FIGURE NO. TITLE PAGE 4.1 Location of Hospital Tengku Ampuan Rahimah, Klang 31 4.2 The old Hospital Tengku Ampuan Rahimah, Klang 32 4.3 The new Hospital Tengku Ampuan Rahimah, Klang 33 4.4 The new Hospital Tengku Ampuan Rahimah, Klang 34 4.5 Biohazard symbol 36 4.6 Clinical waste bin which is filled with tubes 37 4.7 Wheeled clinical waste bin 37 4.8 Clinical waste bin which are clearly labelled 38 4.9 Clinical waste bin which are for sharps 38 4.10 Clinical waste being wheeled into transportation truck 40 4.11 Clinical waste bins being arranged in storage facility 41 4.12 Clinical waste transportation truck 41 4.13 Male to female ratio 43 4.14 Distribution of different age groups 44 4.15 Distribution of years of working of respondents 45 4.16 Percentages of occurrence of accidents related to 45
clinical waste 4.17 Distribution of scope of work of respondents 46 4.18 Awareness towards to the definition of clinical wastes 47 4.19 Awareness of the handling of accidents related to 48

xii
clinical wastes
4.20 Respond to the adherence of the management to 48
standard procedures 4.21 Awareness of the risk exposed to respondents themselves 49 4.22 Awareness of the risk exposed to others (e.g. public) 50 4.23 Familiarity of respondents towards the management plan 50 4.24 Ability of respondents to identify types of clinical wastes 51 4.25 Ability of respondents to segregate, contain and label the 52
clinical wastes
4.26 Awareness of the respondents towards the storage facility 52 4.27 Awareness of the respondents to record keeping 53 4.28 Awareness of the effects of clinical wastes to environment 54 5.1 The amount of patients admitted to the emergency ward 55 5.2 The rate of bed usage in the hospital 56 5.3 The rate of bed capacity being empty from 2001-2005 56
5.4 The rate of birth in Hospital Tengku Ampuan Rahimah 57 5.5 Admission of patients to specialist clinic in Hospital 57
Tengku Ampuan Rahimah from 2001-2004

xiii
LIST OF APPENDICES
APPENDIX NO. TITLE PAGE A Questionnaire form 63 B Clinical Waste Record Sheet 64 C Clinical Waste Transportation Documentation 65

1
CHAPTER I
INTRODUCTION
1.1 Background Study
Clinical waste problems have evolved as the medical and health care services
have evolved. Clinical waste must be given serious attention and properly defined as
an individual waste stream. Control of clinical waste under the law should be
reinforced. The main purpose of this research is to study the current practices
adopted in tackling the hazardous clinical waste. If the clinical waste is not treated
properly, it will pose a serious threat to the human kind.
According to the Ambulance Service Association of UK, clinical waste is
defined as “any waste which consists wholly or partly of human or animal tissue,
blood or other body fluids, excretions, drugs or other pharmaceutical products, soiled
swabs or dressings, or syringes, needles or other sharp instruments, being waste
which, unless rendered safe, may prove to be hazardous to any person coming into
contact with it, and any other waste arising from medical, nursing, dental, veterinary,
pharmaceutical or other similar practice, investigation, treatment care, teaching or
research, or the collection of blood for transfusion, being waste which may cause
infection to any other person coming into contact with it.”

2
1.2 Objectives of research
1. To study and understand the methods and processes of the management and
disposal of clinical waste.
2. To carry out an evaluation on the components of the clinical waste
management system.
3. To identify problems faced by clinical waste management system in the
hospital and clinic and propose ways to improve the system.
1.3 Problem Statement
As the rapid development going on, the heath care institution plays a
significant role in rising human life expectancy. With the rising number of health
care institution, the amount of clinical waste generated will increase at the same time.
Improper management of clinical waste may expose health and safety hazard to
health workers, public and also environment.
Clinical waste is the inevitable part of today’s ever developing and expanding
health care industry. Clinical waste is considered to be the most harmful of every
type of hazardous wastes because of its infectious characteristic. It is necessary to
search for ways to improve the clinical waste management system in order to
minimise or eliminate the harm done by clinical waste to the environment.

3
1.4 Scope of Study
As the research is the case study type, the biggest government hospital in the
district of Klang, Hospital Tengku Ampuan Rahimah is chosen as the case study of
this paper. As much of the development of Malaysia has focused on the central
region, the area of study that has been chosen is Klang Valley.
Site visits will be carried out to the chosen hospitals and clinics to obtain the
relevant information regarding the clinical waste management system. As the clinical
waste management has been handed over to Radicare Sdn Bhd, most of the works
will be dealt with the staffs from the company which has an office at Hospital
Tengku Ampuan Rahimah.
1.5 Significance of Study
The health care is the integral part of human development as it raises human
life expectancy. The aim of this study is to understand the process and methods
involved in treating the clinical waste before it can be disposed of without harming
human and the environment. It is necessary to carry out an evaluation of the
management system to ensure they are competent in handling the clinical waste
management.
This study also aims to identify the inefficiency and ineffectiveness in the
current clinical waste management system in Malaysia. With the site visits and
interviews done in the selected hospital, ways of improving the clinical waste
management system will be proposed.

4
1.6 Expected results
After the research has been carried out, it is expected to achieve the objectives
that have been mentioned above. As this research is not an experiment-oriented type,
hypothesis cannot be established. Even though the expected results cannot be
expressed quantitatively, the desired results will be as follows:
• The flow of process involved in clinical waste management
• An evaluation of the major components of clinical waste management system
• Proposed solutions to solve the problems faced by the clinical waste
management system.

5
CHAPTER II
LITERATURE REVIEW
2.1 Categories of medical waste
Circumstantial waste characterization is of no great importance, due to the
waste stream’s heterogeneity. The focus of concern is on infectious wastes and on
their proper treatment and disposal. Potential infectious wastes, toxic wastes and
potential toxic wastes are classified as wastes that require special handling. [2]
In an attempt to gain a general appreciation of the type of wastes generated in
a hospital, the waste stream of a typical hospital was observed and the following
categories of hospital wastes were recorded, in accordance with similar studies: [2]
• Cultures and stocks of infectious agents and associated biologicals.
• Human blood and blood products
• Pathological wastes
• Contaminated sharps
• Contaminated animal carcasses, body parts and bedding
• Isolation waste
• Wastes from surgery and autopsy
• Contaminated laboratory wastes
• Dialysis unit wastes
• Contaminated equipments

6
Due to the lack of nationally mandated definition of biohazardous waste,
significant definitional changes in the waste stream occur routinely as one crosses
borders between state and local jurisdictions. However termed or defined, proper and
safe management of clinical waste must be an integral part of any heathcare strategy
to protect the safety and health of healthcare providers and support staff, patients and
their families, waste industry workers, and the general public.
Clinical waste is generated primarily in the course of heathcare or research by
both medical institutions and home healthcare activities and to a lesser extent by
illegal drug users. The primary medical institutions generating biohazardous waste
include hospitals, laboratories, physicians, dentists, veterinarians, long-term
healthcare facilities, clinics, blood establishments, and funeral homes.
The following types of waste can be classified and managed as infectious
waste:
• Human blood and blood products
• Cultures and stocks of infectious agents
• Pathological wastes
• Contaminated sharps
• Contaminated laboratory wastes
• Contaminated wastes from patient care
• Discarded biologicals
• Contaminated animal carcasses, body parts, and bedding
• Contaminated equipment
• Miscellaneous infectious wastes

7
2.1.1 Human blood and blood products
Waste human blood and blood products should always be classified and
managed as infectious waste because of the possible presence of infectious agents
that cause blood-borne disease. A major concern today is acquired immune
deficiency syndrome (AIDS), although there are also other blood-borne diseases—
especially hepatitis B—that are serious, debilitating, and sometimes fatal. Due to the
risk that blood-borne diseases could be transmitted by exposure to blood, it is
essential that measures be taken to minimize suck exposures. This includes
minimizing the risk of exposure to blood and blood products in the waste.
Wastes in this category include bulk blood and blood products as well as
smaller quantities suck as the blood samples that are drawn for testing. Since these
wastes are liquid, small quantities of blood are best managed in terms of the
associated container or fomites. Blood-contaminated test tubes, capillary tubes, and
microscope slides and cover slips should be handled together with other sharps.
Blood-soaked bandage fit logically into the category of contaminated wastes from
patient care.
Waste human blood is best treated by steam sterilization or incineration.
After sterilization, the liquid portion can be safely poured off in to a drain. For
management of untreated blood, evaluate the relative hazards of disposals into the
sewer system and of movement through the facility. The first option has the risk of
exposure due to splashing and aerosolisation while the latter option has the risk of
spills with potential for exposure during the spill and its cleanup.

8
2.1.2 Cultures and stocks of infectious agents
Cultures and stocks of infectious agents should always be managed as
infectious wastes because they contain large numbers of infectious microorganisms
at high concentrations. The risk is inherent in cultures from medical, research, and
industrial laboratories. All waste cultures and stocks of infectious agents should be
managed as infectious waste.
It has been general practice to sterilize cultures from medical microbiology
laboratories before disposal. This is done because of the types of infectious agents
that are cultured and the high concentrations of microorganisms present in these
cultures. Steam sterilizers in the laboratory are usually used for sterilizing these
cultures.
One question that may arise is whether these wastes should be sterilized in
the laboratory, elsewhere within the facility, or at an offsite infectious waste
treatment plant. It is best to sterilize culture onsite and right in the laboratory, which
has been common practice. This approach eliminates risk of exposure during
movement of untreated wastes through the facility as well as en route to an offsite
treatment plant. This topic and recommended precautions for use when untreated
wastes must be moved are addressed in the guidelines issued should be followed
strictly.
Selection of appropriate management alternative for your particular facility must
be based on evaluation of the various aspects of the situation. The following
questions are relevant in the decision making process:
• Which infectious agents are present in the waste cultures and stocks? Are
they virulent? Are the diseases that they cause severe? Are they preventable?
Are they treatable?
• Are the infectious agents present in the cultures at high concentrations?
• What type of treatment is most appropriate for this type of waste?

9
• What equipment is available for sterilizing the wastes? Is it located in the
laboratory? Does it have sufficient capacity for treating all the waste cultures
that are generated in the laboratory?
• If there is not sufficient treatment capacity in the laboratory, is other
equipment available elsewhere in the facility? Can the wastes be moved
safely and easily to this location for treatment?
• If the facility has no treatment capability, is there an offsite infectious waste
treatment and disposal option? Does the alternative provide adequate
procedures and safeguards to ensure the safe handling of this type of waste?
2.1.3 Pathological wastes
Pathological wastes are body tissues that are removed during surgery or
autopsy. This category includes tissue samples removed during biopsy, body tissues
and organs, amputated limbs, and body fluids. Special handling of pathological
wastes is warranted for two reasons: the infectious potential of the body tissues and
aesthetic considerations.
Religious beliefs sometimes become the determining factor in the decision on
how to handle these wastes. In some religions, it is important to bury the entire body,
including any body parts that may have been amputated or otherwise removed
surgically. For patients with such beliefs, the body parts should be made available to
the patient or the patient’s family for burial by a mortician.
Otherwise, it is the responsibility of the hospital to dispose of body parts.
Incineration is often the method of choice for pathological wastes because this
technique takes care simultaneously of both potential infectiousness and aesthetics.
Steam sterilization, however, leaves the pathological wastes intact, and the problem
of aesthetics remains. It is not acceptable that recognizable body parts be placed in a
landfill. Therefore, when pathological wastes are steam sterilized, additional
processing is necessary before disposal; options include incineration and grinding of
the sterilized wastes.

10
Another acceptable management alternative for pathological wastes is
handling by a mortician who provides cremation or burial. Many hospitals, especially
those without access to an incinerator, routinely use the services of a mortician for
the disposal of pathological wastes.
2.1.4 Contaminated sharps
The category of sharps includes hypodermic needles and syringes,
intravenous needles, scalpel blades, lances, disposable pipettes, capillary tubes,
microscope slides and cover slips, and broken glass. Contaminated sharps are now
universally recognized as a type of waste requires special handling because of the
double hazard involved—risk of injury and risk of disease. Cuts, scrapes, and
puncture wounds from contaminated sharp can transmit infectious agents through the
skin. The injured person is then at risk for infection and disease, including blood-
borne diseases such as AIDS and hepatitis B.
Sharps are a known occupational hazard to all handlers of medical waste.
Sharps that are tossed loosely in with the trash endanger all who subsequently handle
that waste. There is only one way to prevent injury from sharps; that is to discard
them directly into special containers that confine the sharps and protect against injury.
Use of special containers for discarded sharps would be required by the proposed
rule.
Common features of sharps containers are rigidity, puncture resistance to
retard needle penetration through the wall, narrow openings to prevent retrieval of
discarded needles and syringes, and lockable lid or some other type of locking
mechanism. Specific characteristics of the various sharps containers differ, and it is
possible to evaluate available products to ascertain which one best meets the needs.
In addition to occupational safety and health concerns regarding contaminated sharps,
there are also public health considerations. One concern is the risk to the public from
needles and syringes that appear in public places and degrade the environment.

11
Another concern relates to drug abuse and availability of needles and syringes.
Proper management of sharps can alleviate both concerns. Use of suitable containers
eliminates loose needles and minimizes the risk they pose of needle sticks and other
injuries. Appropriate treatment of sharps makes the needles and syringes unsuitable
for reuse.
Good management policy for sharps eliminates the two hazards in sharps
(infectiousness and physical injury) and prevents their reuse. Incineration
accomplishes these goals simultaneously. After steam sterilization, an additional step
(such as grinding or incineration) is necessary because the needles are still useable
even though they are no longer infectious. Sharps that were not exposed to infectious
agents are not contaminated and, therefore, are not infectious per se. Nevertheless, it
is strongly recommended that treating all sharps uniformly without distinguishing
between those that are contaminated and those that are not.
There are several reasons for adopting a uniform policy for all sharps:
• Although uncontaminated sharps are much less likely to cause disease than
contaminated sharps, there remains the risk of physical injury (cuts, scrapes, and
needle sticks).
• Risk of infection accompanies physical injury by sharps. Even a sterile sharp
discarded into waste becomes non-sterile from being in the waste.
• No one likes to be stuck, and physical injury from sharps is unpleasant. It is also
disturbing to the injured person because of the fear of AIDS it often evokes. The
person is hardly reassured by being told that the particular sharp that cause the injury
was not contaminated because it had not been used on an infected person.
• A uniform sharps policy eliminates decision-making because no one has to
decide whether or not a particular sharp is contaminated.
• Training and management are simpler, easier, and more efficient when all sharps
are handled in exactly the same way.
• Uniform sharps handling means universal use of sharps containers, a practice that
offers protection for all handlers of sharps.
• A uniform sharps handling policy is consistent with public health concerns about
drug abuse and the reuse of needles and syringes.

12
2.1.5 Contaminated laboratory wastes
The category of contaminated laboratory wastes includes all potentially
infectious wastes generated in microbiological, pathological, medical, research, or
industrial laboratories that are not classified as another type of infectious waste (such
as cultures, blood, or sharps). Before the advent of disposable laboratory supplies,
used materials were routinely sterilised before reuse. With the introduction of
disposables, these items became wastes that were generally discarded directly into
the trash.
Contaminated laboratory waste is one of the waste categories termed
optionally infectious by EPA. All laboratory wastes should be evaluated for potential
infectiousness using professional judgment. Those wastes that are determined to be
potentially infectious should be managed as infectious waste.
Examples of contaminated laboratory wastes include:
• Specimen and culture containers such as cups, bottles, flasks, petri dishes,
and test tubes.
• Implements used to manipulate infectious materials such as specimen and
cultures (for example, swabs, spreaders and pipettes)
• Components of diagnostic kits that are contaminated by use with specimens
• Personal protective equipment such as disposable gloves, lab coats, aprons,
and masks that are grossly contaminated with blood, body fluids, secretions,
excretion, or cultures.
Some of these items belong in other infectious waste categories. For example,
Sharps from laboratories should be handled in accordance with the special
procedures established for handling of all sharps, and cultures should be managed
like wastes in that particular category.

13
Contaminated laboratory wastes can be treated by any treatment technology
that provides effective treatment of the waste. No particular treatment is best for all
these wastes.
2.1.6 Contaminated wastes from patient care
Contaminated wastes from patient care originate from various areas of patient
care other than laboratories, such as clinics, patient rooms, emergency rooms,
operating rooms, hemodialysis centres, and morgues. This category includes all
potentially infectious wastes that do not belong to other specific categories such as
blood and body fluids, cultures or sharps.
A general guide for determining which wastes from patient care are
potentially infectious is to include in this category all wastes that are grossly
contaminated with blood, body fluids, excretions, and secretions. This policy is
consistent with the CDC recommendations for universal precautions. Wastes from
general patient care include such diverse items as diapers and bed pads, intravenous
tubing, catheters and bags, drainage tubing and pouches, and wet dressings
(especially those soiled with blood, pus, or body fluids).
Current management practices for wastes from surgery and autopsy vary
greatly. In some hospitals, all wastes from surgery are handled as infectious. In
others, surgical cases are classified as either “clean” or “dirty” and only the wastes
from dirty cases are considered infectious. Obviously, the decision is an individual
one that is affected by the outlook and perceptions of risk at each individual hospital.
Wastes from hemodialysis that have been grossly soiled by contact with patient
blood should be managed as infectious waste. This includes disposable tubing, filters,
towels, aprons, gloves and lab coats. Classifying wastes from patient care as
infectious or not infectious is a decision based on judgment. There are three
alternatives:

14
• Wastes that should never be managed as infectious
• Wastes that should always be managed as infectious
• Wastes that require individual evaluation
There is a general guide for classifying wastes from patient care. The difference
between “always infectious” and “sometimes infectious” depends on how it is
distinguished between “grossly contaminated” and “slightly contaminated”. It is a
matter of personal evaluation and decision-making that requires professional
judgment: input from the infection control practitioner is helpful. Infectious wastes
from patient care can be treated by any treatment technology that is effective. No
particular treatment technique is best for all these wastes.
2.1.7 Discarded Biologicals
This category of infectious wastes is comprised of waste biologicals, such as
live and attenuated vaccines. Included are production wastes as well as products that
are discarded for various reasons (quality control, recalls, outdating). Note that many
wastes from production of biologicals are covered by other categories of infectious
waste such as cultures and stocks of infectious agents, sharps, contaminated
laboratory wastes, and contaminated animal carcasses, body parts, and bedding.
Discarded biologicals are usually incinerated. Incineration not only treats the
infectiousness, it also destroys the materials as well as the labels. These are important
considerations for the manufacturer. Production wastes, like other infectious wastes,
can be treated by any technique that is effective. Heat sterilisation and chemical
disinfection are often appropriate for liquid wastes.

15
2.1.8 Contaminated animal carcasses, body parts and bedding
In some research projects, animals are infected with human pathogens in
order to study disease processes and the efficacy and side effects of pharmaceuticals.
The wastes from such research (that is, the animal carcasses, body parts, and
bedding) are best handled as infectious waste so as to minimise the risk of exposure
for waste handlers.
Animal carcasses and body parts should be handled like pathological waste.
Animal bedding can be difficult to treat—bedding material is a good insulator that
can impede steam sterilisation, and its high moisture content can prevent complete
combustion during incineration. It is important to standardise and to validate
treatment procedures and then to follow the established procedures in order to be
certain that treatment will be effective.
2.1.9 Contaminated equipment
Equipment and equipment parts are discarded when no longer useful because
they cannot be repaired or they have become obsolete. Equipment may have been
contaminated with infectious agents (for example, by spills and splashing) during use,
and prudent management provides for decontamination of the equipment before it is
actually thrown out. Therefore, from the safety perspective, contaminated equipment
should be managed as infectious waste.
Usefulness is not a consideration with equipment that is being junked. If
practical, steam sterilisation or incineration could be used for treatment because the
effect of steam or combustion does not matter when the equipment will not be used
again. For contaminated equipment that is large ( such as centrifuge), the best
approach may be to treat the object using formaldehyde decontamination before it is
moved.

16
2.1.10 Miscellaneous infectious wastes
This category includes general types of infectious waste that are not readily
assigned to another specific category. These wastes are usually generated in the
handling of infectious materials and wastes. Personal protective equipment should be
worn whenever and wherever potentially infectious materials and wastes are handled.
These items are usually disposable. They include latex gloves, masks, aprons, and
lab coats—some or all of which may be appropriate for use under particular
circumstances. Also in this category is the waste that is generated during cleanup of
spills of infectious materials and wastes. These wastes include absorption materials
(loose materials as well as spill pillows), towels, mops, torn or broken containers,
and the personal protective equipment that was worn during the cleanup.
2.2 Medical waste management
In general, the key elements to an effective medical waste management programme
should include:
• Management plan
• Definition
• Identification
• Segregation, containment and labeling
• Storage
• Treatment
• Transportation ( on-site and off-site)
• Disposal
• Contingency planning
• Monitoring and record keeping
• Staff training

17
2.2.1 Management plan
Central to a facility’s medical waste management programme is the medical
waste management plan. In the plan should be documented information describing
all aspects of the waste management programme from the point of waste generation
to final disposal. Written plans should be prepared by both larger generators such as
hospitals and smaller generators such as dentists, although the plans of smaller
generators may only need to be one or two pages in length. Nevertheless, the
exercise of writing a plan, large or small, focuses attention on how waste is managed
by a facility and documents step-by-step how waste management is to be carried out.
A written plan also provides a written record should one ever become necessary.[1]
Once written, the plan should be reviewed periodically and updated as necessary,
and should be made readily available to all employees involved in waste
management activities. The plan should be written in a format that is easily
understood, maintained as a working document by the facility, and be available for
inspection by government regulators and the public if requested. The plan should
address:[1]
• Compliance with applicable regulations
• Responsibilities of all involved staff (e.g., infection control members,
environmental control and housekeeping personnel, department and
individual responsibilities)
• Definition of all medical wastes handled within a facility
• Procedures for medical waste management, including:
Identification
Segregation
Containment
Labeling
Storage
Treatment
Transport
Disposal
Monitoring and record keeping

18
Contingency planning
• Training for all involved staffs (professional, medical, environmental services,
housekeeping, etc.)
2.2.2 Identification
Once the medical waste stream has been defined, the next step is to conduct an
audit of the waste stream. Before a management strategy can be developed, the
medical waste team must identify:
• Location of waste generated
• Types and amounts (volume or weight) of waste generated
Lists identifying types and amounts (either in volume or weight, depending on
how disposal costs are based) of waste generated should be developed for each
location where medical waste is generated. By documenting location of waste
generation, types, and amounts generated, informed management decisions can be
made.
2.2.3 Segregation, containment, and labeling
In general, medical waste should be segregated from the general waste stream
at the point of origin by the generator of the waste into clearly marked containers that
take into consideration the waste type (e.g., liquid wastes, non-sharp/non-liquid
wastes, sharp wastes). To contain costs, facility staff should be trained to segregate
only that which has been specifically defined as medical waste by the facility.
Casual disposal of nonbiohazardous waste materials can dramatically increase a
facility’s waste disposal costs. Segregation should be carried at source. [8]
19
Non-sharp biohazardous wastes (solid/semisolid wastes) should be segregated
into disposable leak-proof containers or plastic bags that meet specific performance
standards. The bags should also be constructed so as to preclude clipping, tearing, or
bursting under normal use. These bags should be tagged or effectively marked by the
generator as containing medical waste. The bags should be secured to prevent
expulsion of contents during handling, storage or transport. Liquid medical waste
should be prevented from entering these bags.
Sharp wastes (e.g., hypodermic needles) should be contained in rigid, leak-
proof, puncture-resistant, break-resistant containers that can be tightly lidded during
storage, handling or transport. The most suitable container material would be plastic.
Liquid medical waste should be segregated into leak-proof containers that are
capable of transporting wastes that have been packaged as described, additional
protection should be provided to the original containers (plastic bags, sharp
containers, liquid containers) by placing them into other durable containers, such as
disposable or reusable pails, cartons, boxes, drums, or portable bins.
If containers are to be reused for medical waste storage, handling or transport,
they should be thoroughly washed and decontaminated by an approved method each
time they are emptied unless the surfaces of the containers had been protected by
disposable liners, plastic bags, or other means. The process of cleaning should
include agitation (scrubbing) to remove any visible solid residue, followed by
disinfection. Disinfection could be accomplished using chemical disinfectants. These
containers should not be used for any other purpose unless they have been properly
disinfected and have had biohazardous waste symbols and labels removed.

20
2.2.4 Storage
Facilities that store medical wastes should have a specific storage area for
that purpose. The storage area should be inaccessible to unauthorised entry. The area
should offer protection from animals, the elements (e.g., rain and wind), and should
not provide a breeding place or a food source for insects or rodents. Storage time and
temperature should be considered due to putrefaction of the waste with time.
Microorganisms will grow and decompose the waste in storage, creating the
unpleasant odors associated with putrefaction or rotting garbage.
2.2.5 Treatment
Medical waste treatment options are available either on- or off-site,
depending on the facility’s needs and budget. Options include incineration, steam
sterilisation, and various alternatives treatment technologies, including microwave
irradiation, electrothermal deactivation, chemical treatment, or ionising radiation.
2.2.6 Transportation
Transport of biohazardous waste must be considered as the waste moves
through the facility to storage areas, and if the waste is to be transported off-site to a
treatment/disposal facility. Carts used to transport waste within a facility from the
point of generation to the storage site should be used only for that purpose and not
for other purposes (e.g., foot carts and miscellaneous equipment transfers). Carts
should be cleaned and disinfected routinely.
Off-site transportation must meet requirements established by the relevant
authorities and all state and local transportation requirements relating to inter- and
intrastate transport of medical waste. In general, the waste destined for off-site
21
transport should be transported only in leak-proof and fully enclosed containers or
vehicle compartments. Biohazardous wastes should not be transported in the same
vehicle with other waste or medical specimens unless separately contained.
Biohazardous waste spills should be decontaminated promptly. The waste should
only be transported to a treatment facility that meets all local, state, and federal
environmental regulations.
2.2.7 Record keeping
Accurate record keeping provides an essential history of a facility’s waste
management practices. Waste management records represent a document or practices
that can be used by the facility to make informed waste management decisions.
Records are essential for demonstrating compliance with environmental and public
health requirements. Accurate records are also essential in terms of potential liability
protection should it ever become necessary. To see the importance of this, one only
has to look at the plight of many waste generators of two decades ago who are now
faced with huge cleanup cost settlements under the current regulations, due to past
largely undocumented waste management practices.
2.2.8 Staff training
The medical waste management plan should address specific training and
educational needs for professional staff and housekeeping/custodial staff. Training
should include:
• An explanation of the waste management plan
• Assignment of roles, responsibilities, and expectations
• Risks associated with the waste management work environment
• The location and proper use of personal protective equipment

22
• Components of the waste management system (waste identification,
segregation, containerisation, labeling, transport, treatment and disposal)
• Regulations and the consequences of failing to comply (regulatory
enforcement consequences)
• Procedures to follow should a needle stick or other exposure occur
Training should be conducted following development and implementation of
the management plan, when new employees are hired, whenever management
practices change, and as a periodic refresher.
2.3 Clinical waste laws and regulations
Hazardous waste management is one of the more dynamic areas of
Malaysia’s environmental regulatory regime. Article 34B of the Environmental
Quality Act ("EQA") serves as the legal basis for the nation’s hazardous
("scheduled") waste management regime. Among other provisions, Article 34B
specifies that "[n]o person shall…place, deposit or dispose of, or cause or permit to
place, deposit or dispose of, except at prescribed premises only, any scheduled
wastes on land or into Malaysian waters [without appropriate prior written
approval]." The Minister of the Ministry of Science, Technology and the
Environment ("MOSTE") is empowered under Articles 21 and 51 to specify
conditions (through subsidiary legislation) for the discharge or deposit of wastes,
including provisions regarding the designation or "set aside" of areas within which
such activities are prohibited or restricted. Persons violating the measures in Article
34B are subject to penalties not exceeding 500,000 Malaysian ringgit (roughly US
$131,575), and/or imprisonment terms. A further discussion of the EQA, including a
link to the full text of the unofficial English version, is included under the Product
Take-Back and Recycling section of the Malaysia Country Page.

23
Detailed implementing provisions concerning waste classification, labeling,
treatment, disposal, and related activities are contained in subsidiary legislation. Key
subsidiary legislation for purposes of understanding Malaysia's hazardous waste
classification scheme includes the Environmental Quality (Scheduled Wastes)
Regulations 1989 ("Regulations"). Additional information on the hazardous waste
container labeling provisions of the Regulations is provided under the Packaging and
Labeling section of the Malaysia Country Page.
Although outside the scope of the tracking project at this time, EIA members
may also wish to note subsidiary legislation under the EQA governing waste
treatment and disposal. This legislation includes:
- The Environmental Quality (Prescribed Premises) (Scheduled Wastes
Treatment and Disposal Facilities) Order 1989; and
- The Environmental Quality (Prescribed Premises (Scheduled Wastes
Treatment and Disposal Facilities) Regulations 1989

24
CHAPTER III
METHODOLOGY
3.1 Literature review
A literature review is a body of text that aims to review the critical points of
current knowledge on a particular topic. Most often associated with science-oriented
literature, such as a thesis, the literature review usually precedes a research proposal,
methodology and results section. Its ultimate goal is to bring the reader up to date
with current literature on a topic and forms the basis for another goal, such as the
justification for future research in the area. A good literature review is characterised
by: a logical flow of ideas; current and relevant references with consistent,
appropriate referencing style; proper use of terminology; and an unbiased and
comprehensive view of the previous research on the topic. A literature review is a
piece of discursive prose, not a list describing or summarizing one piece of literature
after another.
All of the data and information concerned are collected from the relevant
parties and libraries. An in-depth investigation is carried out based on the
information gathered to understand the methods and processes involved in the
clinical waste management and disposal. The evaluations of the management system
in the clinical waste management are obtained from the relevant survey.

25
3.2 Site Visit
All the preparations are arranged to visit the hospital and clinic involved to
carry out the case studies. The standard procedures of handling clinical wastes are
observed carefully and closely. A tour of all the facilities and infrastructure from the
point of waste generation right up to the disposal of waste is desired. An officer from
the relevant department is requested to answer questions concerning the clinical
waste management. A checklist is prepared before the visit to ensure the hospital and
clinics comply with the laws and regulations.
3.3 Interview
Some interviews will be conducted to get a more in-depth view at the clinical
waste management system. The department in charge will be subjected to some
question and answer sessions. The aim of this method is to know the problem faced
by the current clinical waste management system. The staffs will also be asked to
recommend ways to improve the system. The recommendations proposed will be
reviewed to come up with the best way to ensure that the clinical waste management
system is more efficient.
An interview is a conversation between two or more people (The interviewer
and the interviewee) where questions are asked by the interviewer to obtain
information from the interviewee. Interviews can be divided into two rough types,
interviews of assessment and interviews for information. The interview method
adopted for this research will be interviews for information.

26
3.4 Questionnaire
A questionnaire is carried out to conduct the case study as to find out how
effective the clinical waste management is at the hospital. The questionnaire is
targeted at the staffs from the lowest to highest rank in the administration of the
health care facilities. A list of question is compiled based on the literature review
carried out and the sample is ensured to be random to obtain accurate statistic.
A questionnaire is a research instrument consisting of a series of questions
and other prompts for the purpose of gathering information from respondents.
Although they are often designed for statistical analysis of the responses, this is not
always the case.
Questionnaires have advantages over some other types of surveys in that they
are cheap, do not require as much effort from the questioner as verbal or telephone
surveys, and often have standardized answers that make it simple to compile data.
However, such standardized answers may frustrate users. Questionnaires are also
sharply limited by the fact that respondents must be able to read the questions and
respond to them. Thus, for some demographic groups conducting a survey by
questionnaire may not be practical.
Questionnaires are frequently used in quantitative marketing research and
social research in general. They are a valuable method of collecting a wide range of
information from a large number of respondents. Good questionnaire construction is
critical to the success of a survey. Inappropriate questions, incorrect ordering of
questions, incorrect scaling, or bad questionnaire format can make the survey
valueless. A useful method for checking a questionnaire for problems is to pretest it.
This usually involves giving it to a small sample of respondents, then interviewing
the respondents to get their impressions and to confirm that the questions accurately
captured their opinions.

27
Components of the survey constructed to conduct the search are consist of
gender, age, years of working , scope of work and history of accidents related to
clinical wastes. Lastly, a list of scaled questions is prepared to gauge the awareness
among the staffs to the clinical waste management system.
3.4.1 Gender
Gender in common usage refers to the distinctions between masculinity and
femininity. This question will establish the percentage of male and female
participants of the survey. The relationship between gender and the rest of the
structure of the survey will be established to determine whether there is a link. If the
link is determined, some deduction can be made regarding to the occurrence of the
phenomenon. Currently, anthropologists, sociologists, psychologists, and gender
theorists suggest that gender is a social construction, that that one is always in the
process of becoming a gender rather than actually being a gender.
3.4.2 Age
Age is the length of time a human has lived. Age is usually associated with
wisdom as a person gains precious experience as he live his life. This question will
determine the basic demographic of the sample group which participates in the
survey. The senior staffs will be more familiar with the management system as they
are in the healthcare service in a longer period of time. Their wisdom prove to be
invaluable to the hospital as they are needed to train new staffs.

28
3.4.3 Years of working
The amount of period a staff has been working in the hospital differs in the
sample group which participates in the survey. The correlation between the years of
working with the structured questions will give a glimpse into how well or organised
the clinical waste management is. The experience one gains will ensure the
efficiency and effectiveness of the system.
3.4.4 Scope of work
The major scopes of work that has been identified are doctor, nurse and
administrator. As they work in different departments, their exposures to clinical
waste differ largely. For example, an administrator may not know that much about
clinical waste segregation as compared to a nurse. It is hoped that with this
component of survey, the correlation between it and the rest of the survey will give
us insights into the management system thoroughly.
3.4.5 Scaled questions
A list of scaled questions has been prepared to enquire the respondents
regarding to the clinical waste management practices. The questions have covered all
of the aspects of the clinical waste management system from the identification to
disposal. The questions are as follows:
1. I have the knowledge of the definition of clinical waste
2. My training is sufficient to deal with any accident with clinical waste spills
3. Clinical waste management follows the standard procedure
4. I am aware of danger exposed to myself by the clinical wastes
5. I am aware of the danger exposed to others by the clinical wastes
6. I am familiar with the clinical waste management plan by the hospital

29
7. I am able to identify various type of clinical wastes
8. I know how to segregate, contain and label the clinical wastes properly
9. I know the location of the storage area of the clinical wastes
10. Record keeping of the clinical wastes is done properly
11. I am aware of the effects of the clinical wastes to the environment
The type of scale being employed in this survey is Likert scale. A Likert scale
(pronounced 'lick-urt') is a type of psychometric response scale often used in
questionnaires, and is the most widely used scale in survey research. When
responding to a Likert questionnaire item, respondents specify their level of
agreement to a statement. The scale is named after Rensis Likert, who published a
report describing its use.
A typical test item in a Likert scale is a statement. The respondent is asked to
indicate his or her degree of agreement with the statement or any kind of subjective
or objective evaluation of the statement. Traditionally a five-point scale is used,
however many experts advocate using a seven or nine point scale. Likert scaling is a
bipolar scaling method, measuring either positive or negative response to a statement.
Sometimes Likert scales are used in a forced choice method where the middle option
of "Neither agree nor disagree" is not available. Likert scales may be subject to
distortion from several causes. Respondents may avoid using extreme response
categories (central tendency bias); agree with statements as presented (acquiescence
bias); or try to portray themselves or their organization in a more favorable light
(social desirability bias).

30
CHAPTER IV
RESULTS AND ANALYSIS
4.1 Introduction
In this chapter, the analysis of the results will be divided into two parts: first
is discussing the clinical waste management system being utilised by the case study
subject (Hospital Tengku Ampuan Rahimah) and the second part will be the analysis
of the survey carried out to gauge the awareness among the staffs to the system
mentioned.
4.2 Clinical waste management
In this first part of the analysis of the results, the clinical waste management
system will be explained in details from the point of generation of the wastes right
up to the disposal stage. It should be noted that the much of the management aspect
is being handled by the concessionaire in charge of hospitals in the central region
which is known as Radicare (M) Sdn Bhd.

31
4.2.1 Background of hospital
Hospital Tengku Ampuan Rahimah has started its operations since April
1985. It is a government hospital with the capacity of over 800 beds and 20 clinical
fields. It is situated at the southern region of Klang district. The hospital provides
major medical services and top of the class healthcare professionals. This hospital is
the main reference for Klang district and the surrounding districts which include
Sabak Bernam, Petaling, Kuala Langat, Kuala Selangor and Sepang.
This hospital also concentrates on ambulance service and is equipped with a
helicopter flight route for emergency transfer. It acts as the training centre for
medical students from Universiti Malaya. Even with the emergence of new hospitals
such as Hospital Putrajaya, Hospital Serdang and Hospital Selayang, statistics have
shown an increase of patience admission from year to year. The year of 2005 marks
the admission of 80,112 patients compared to the admission of 76,553 from the
previous year which is an increase of 4.65 percent.
Figure 4.1: Location of Hospital Tengku Ampuan Rahimah, Klang, Selangor

32
The hospital for Klang district was built in the 1890s on a small hill near to
the government and business buildings. The first District Surgeon to the Coast
District who was responsible of the hospital was Dr Watson followed by Dr. Reid
and subsequently Dr Gerrard and Dr Millard. On 1st January 1976, the hospital was
upgraded to Klang General Hospital and was headed by a medical administrator.
According to the statistics from 1901, there were 2789 out-patients and 1822 in-
patients being treated at the hospital. During that period of time, cases such as
diarrhoea, respiratory illness and paediatric illness were the major cases being treated.
Figure 4.2 : The old Hospital Tengku Ampuan Rahimah, Klang
Due to the ageing of the original buildings and rising needs of the increasing
patients as well as the introduction of new healthcare services, a new hospital was
built on a land of 25.5 hectare with the cost of RM68.5 million. Phase I of the
construction commenced on 1 June 1979. Phase II began on 27 October 1981 and
finished on February of 1985. The hospital is named Hospital Tengku Ampuan
Rahimah and the opening was officiated by DYMM Sultan Salahuddin Abdul Aziz

33
Shah Alhaj on 2 September 1985. The hospital building consists of 9 storeys and is
situated 3 km from Klang town centre.
Figure 4.3: The new Hospital Tengku Ampuan Rahimah, Klang Transfer of the patients to the new hospital started on April 1985. At the
beginning, it had 27 wards and 750 beds capacity and now has increased to 29 wards
and 831 beds capacity. The hospital is headed by Director, Deputy Director (medical)
and Deputy Direct (management). This hospital acts as a facility to a population of
409,994 people, especially to the residents of Klang city. It also prepare specialist
service to cases referred from Hospital Banting, Tanjung Karang and Sabak Bernam
and also private clinics as well as private medical centres.
34
Figure 4.4: The new Hospital Tengku Ampuan Rahimah, Klang
4.2.2 Processes of clinical waste management system
From the research that has been conducted at the hospital chosen as the case
study, the main parties involved are the hospital itself and a concessionaire known as
Radicare Sdn Bhd. There used to be an incinerator in the hospital but the operation
had stopped since the service was outsourced to Radicare Sdn Bhd after the
privatisation began at 1996 [9]. Basically, the processes of the management system
are broken down into identification and segregation, labelling and packaging,
internal transportation, storage, external transportation. All of the clinical wastes
were transported to the incinerator at Tg. Panglima Garang for the treatment and
disposal phase.
4.2.2.1 Identification and Segregation
It is the duty and responsibility of the healthcare staffs to identify and
segregate the clinical wastes when they are generated. It is paramount task

35
considering the amount of wastes generated daily from different wards. It is essential
that the clinical wastes need to be separated from household wastes as it will increase
the volume of the wastes and also the workload later. Furthermore it will increase the
cost of the treatment.
Table 4.1: The different groups for segregating the clinical wastes
Group Types of clinical waste
Group A • Soiled surgical dressing, cotton wool, gloves, swabs and all
other contaminated waste from treatment areas, plaster and
bandaging which have come into contact with blood or
wounds, cloth and wiping material used to clean up body fluids
and spills of blood.
• Material other then linen from cases of infectious disease (e.g.
human biopsy material, blood, urine, stools)
• All human tissue (whether infected or not), limbs, placenta,
animal carcasses and tissue from laboratories and all related
swabs and dressings.
Group B • Sharps such as discarded syringes, needles, cartridges, broken
glass, scalpel blades, saws and any other sharps instrument that
could cause a cut puncture.
Group C • Clinical waste arising from laboratories (e.g. pathology,
haematology and blood transfusion, microbiology, histology)
and post mortem room waste, other than waste included in
Group A
Group D • Pharmaceutical wastes such as expired drugs, vaccines an sera,
including expired rugs that have been returned from ward, drug
that have been spilled or contaminated, or are to be discarded
because they are no longer required
• Cytotoxic drugs
Group E • Used disposable bed-pan liner, urine containers, incontinence
pads and stoma bags.
36
4.2.2.2 Labelling and packaging
Standard code of colour is used for every plastic bags and plastic containers
for the purpose of packaging. Each of the plastic bag is labelled with a biohazard
symbol and it is an obligation under Environmental Quality Act (Scheduled Waste)
1989 in Third Schedule, (Regulation 8).
Table 4.2: Different colour code for the purpose of packaging Colour Type of waste
Black Household waste
Yellow Clinical waste to be disposed by incinerator
Light Blue Clinical waste from high risk disease
A biological hazard or biohazard is an organism, or substance derived from
an organism, that poses a threat to (primarily) human health. This can include
medical waste, samples of a microorganism, virus or toxin (from a biological source)
that can impact human health. It can also include substances harmful to animals. The
term and its associated symbol are generally used as a warning, so that those
potentially exposed to the substances will know to take precautions.
Figure 4.5: Biohazard symbol

37
Figure 4.6: Clinical waste bin which is filled with tubes
Figure 4.7: Wheeled clinical waste bins

38
Figure 4.8: Clinical waste bin which are clearly labelled
Figure 4.9: Clinical waste bins which are for sharps.

39
4.2.2.3 Internal Transportation
Radicare Sdn Bhd will dispatch porters to the different wards of the hospital
to collect the clinical wastes that have been segregated by the healthcare staffs. The
main equipment employed during the internal transportation process is the wheeled
bin. It eases the work of the porter and improves the safety aspect. All of porters are
equipped to wear self protection gear before they perform their duties. The self
protection gear consists of head scarf, gloves, mask and apron which are white in
colour. The porter will tie up the plastic bags containing clinical waste and put them
inside the wheeled bin. A document known as clinical waste record sheet is filled up
with details such as type of clinical waste, date and time of collection and is signed
by the staff on duty in the ward. The document which is on a sticker is pasted on the
plastic bags.
4.2.2.4 Storage
All of the clinical wastes collected will then be transported to the temporary
storage facility situated within the premise of the hospital. Proper storage is
imperative due to hazard and harm to public and environment. The considerations of
designing the storage largely depend on several factors. These factors act as general
guideline when installing the storage area for the purpose of hazardous wastes.
The factors are as below:
a. The amount of space available on the site
b. The training and experience of the staff
c. The security of the site
d. The emergency plans available

40
4.2.2.5 External Transportation
The function of external transportation is to move the clinical waste from the
temporary storage facility to the incinerator which is situated at Teluk Panglima
Garang, Banting. The vehicle is specially designed for carrying clinical wastes. The
inner space of the vehicle storage is layered by stainless steel and aluminium to give
smooth surface for cleaning purposes. Every hole and pores inside it must be closed
to prevent the waste from sticking and left behind during the unloading and cleaning
process. The vehicle cannot be used for any other purposes.
In HTAR, Radicare Sdn Bhd will send a vehicle from the incinerator plant to
collect the clinical wastes daily. The reason behind this is the temporary storage
facility does not have cold storage feature and the wastes cannot be stored for long
under normal temperature.
Figure 4.10: Clinical wastes being wheeled into transportation truck

41
Figure 4.11: Clinical waste bins being arranged in storage facility
Figure 4.12: Clinical waste transportation truck
42
4.2.2.6 Incineration
Generally, the incinerator in Teluk Panglima Garang has four different stages.
Each of the stage is designed to convert solid wastes into gaseous, liquid and solid
while reducing environmental impacts of the incinerator [13]
a. Charge End (Feeding)
The workers will load the 15 kg wheeled bins into skip loader. Then, the
wastes are discharged into hopper. The feed conveyor will move the wastes
into ram feeder. Finally, the wastes are pushed into rotary kiln for
incineration.
b. Thermal Stage
The thermal stage is consists of Primary Combustion Chamber (PCC) and
Secondary Combustion Stage (SCC). PCC employs rotary kiln for the first
incineration stage. Rotary kiln is insulated with castable or fire brick that can
hold the temperature of 760°C to 900°C. 130% to 150% of excess air is
required to complete the combustion. SCC employs vertical tower as method
of incineration. The function of SCC is to disperse dioxin molecule at 1000°C.
c. Heat Recovery Stage
In this stage, hot air from SCC-Down Leg will enter waste heat boiler. Waste
heat boiler is a cooling media to reduce the temperature of hot air. The excess
steam is used to wash wheeled bins.
d. Pollution Control Stage
Air containing toxic and acid gas from heat recovery stage is treated using
powdered lime and carbon. Hydrated powder lime will neutralise acid gas in
recommended reacting temperature of 160°C to 180°C. Activated carbon is
used to treat heavy metal content.

43
4.3 Analysis of the survey
The purpose of the analysis is to gauge the awareness among the respondents
who consist of the staffs of the HTAR towards the clinical waste management system.
The first part of the questionnaire is made up of questions regarding the demographic
pattern and working background of the respondents. The second part which consists
of scaled question is used to find out how far is the awareness among the staffs
towards to the components of the clinical waste management system such as
segregation, documentation and storage.
4.3.1 General questions analysis
From the analysis carried out based on the survey forms which have been
collected back from the respondents, the female staffs are the majority of the sample
group. Female is the majority who work as healthcare staffs such as nurse. Nurses
usually have a higher frequency of handling clinical wastes.
Male to Female Ratio of respondents
20%
80%
Male Female
Figure 4.13: Male to Female Ratio of respondents
44
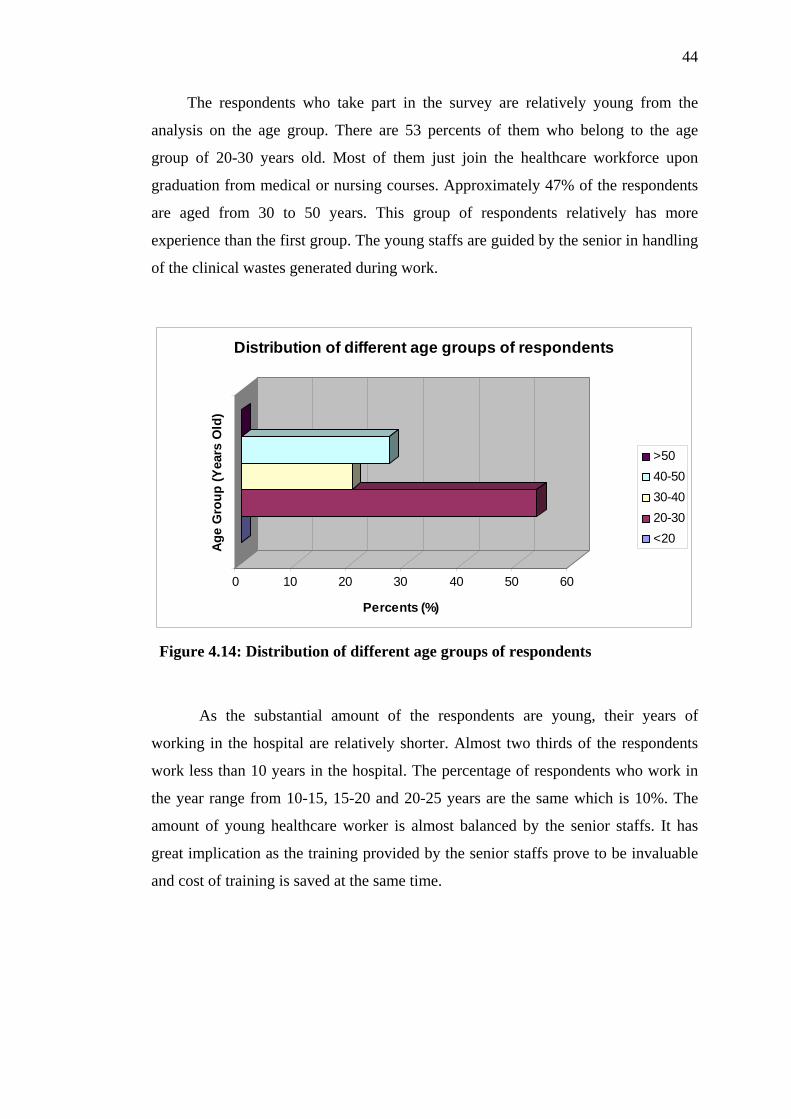
The respondents who take part in the survey are relatively young from the
analysis on the age group. There are 53 percents of them who belong to the age
group of 20-30 years old. Most of them just join the healthcare workforce upon
graduation from medical or nursing courses. Approximately 47% of the respondents
are aged from 30 to 50 years. This group of respondents relatively has more
experience than the first group. The young staffs are guided by the senior in handling
of the clinical wastes generated during work.
0 10 20 30 40 50 60
Percents (%)
Age
Gro
up (Y
ears
Old
)
Distribution of different age groups of respondents
>5040-5030-4020-30<20
Figure 4.14: Distribution of different age groups of respondents
As the substantial amount of the respondents are young, their years of
working in the hospital are relatively shorter. Almost two thirds of the respondents
work less than 10 years in the hospital. The percentage of respondents who work in
the year range from 10-15, 15-20 and 20-25 years are the same which is 10%. The
amount of young healthcare worker is almost balanced by the senior staffs. It has
great implication as the training provided by the senior staffs prove to be invaluable
and cost of training is saved at the same time.

45
0
10
20
30
40
50
60
70
Percents (%)
Years
Years of working of the respondents
<1010-1515-2020-2525-30>30
Figure 4.15: Distribution of years of working of the respondents
Regarding to the question about the history of occurrence of accidents related
to clinical wastes, around 83% of the respondents give negative answer whereas 17%
of them answer positively. This proves that the track record of the hospital is
outstanding in their handling of clinical wastes. From the oral answers given by those
who answer positively, the accidents are minor in nature
Percentages of occurence of accidents related to clinical wastes
17%
83%
YesNo
Figure 4.16: Percentages of occurrence of accidents related to clinical wastes

46
The final question of the general category of the questionnaire is asking about
the scope of work by the respondents. The doctors and nurses made up 40% of the
sample group respectively. The rest of them work as administrator in the office or
therapists who rarely need to deal with clinical wastes. The awareness among the
doctors and nurses are the most significant as they are the ones who deal with clinical
waste more frequently than others in the group.
Distribution of scope of work of respondents
0 10 20 30 40 50
Scop
e of
wor
k
Percents (%)
OthersAdministratorDoctorNurse
Figure 4.17: Distribution of scope of work of respondents

47
4.3.2 Scaled questions analysis
The first question ask about the respondent’s knowledge regarding to the
clinical wastes. As it is shown in figure 4.6, around 70% of them agree that they
possess the basic knowledge to define clinical wastes. As most of them just graduate
from medical or nursing courses, the knowledge is still fresh in their mind. Even
though the knowledge of the clinical wastes is vital, it is through day-to-day work
experience that one gain a deeper sense on this subject.
Awareness towards to the definition of clinical waste
0 3 7
70
20
0
10
20
30
40
50
60
70
80
Scale of response
Perc
ents
(%) Strongly Disagree
DisagreeNeitherAgreeStrongly Agree
Figure 4.18: Awareness towards to the definition of clinical waste.
The next question is to gauge their readiness in handling any accidents related
to clinical wastes such as spills or exposure. From the chart 4.7, 63% of them agree
that they have the sufficient training in handling any accidents arise from clinical
wastes. However, 17% disagree and 13% answer neither on this question. This shows
that training is still needed to teach about the emergency plan should any accident
happens.

48
Awareness towards the handling of accidents related to clinical wastes
3
17 13
63
3
0
10
20
30
40
50
60
70
Response
Perc
ents
(%) Strong Diagree
DisagreeNeitherAgreeStrongly Agree
Figure 4.19: Awareness of the handling of accidents related to clinical wastes
On the question regarding to whether the hospital’s clinical waste
management plan adheres to the standard procedure outlined by relevant
organization, 56% of the respondents agree and 20% of them strongly agree with the
statement. It can be deduced from the analysis of figure 4.8 that the management
plan outlined by the hospital follows the standard procedure properly. It is one of the
most important elements in the clinical waste management system.
Respond to the adherence of management to standard procedures
0%
7%
17%
56%
20%
Strongly DisagreeDisagreeNeitherAgreeStrongly Agree
Figure 4.20: Respond to the adherence of management to standard procedures

49
The following two questions are related in some way as they gauge the
respondent’s awareness of the risk exposed by the clinical wastes during the handling
process. On the statement on whether they understand the risk exposed to themselves,
43% of them strongly agree and 47% of them agree with it. Understanding of such
risk will increase their alertness in handling clinical wastes and this will improve the
efficiency of the system.
Awareness of the risk exposed to the respondents themselves
0% 10%0%
47%
43%
Strongly DisagreeDisagreeNeitherAgreeStrongly Agree
Figure 4.21: Awareness of the risk exposed to respondents themselves
37% of them strongly agree and 50% of them agree with the question
regarding to their understanding of the risk exposed by the clinical wastes to others
such as patients or public. The awareness of such risk should be incorporated into
their mind as they need to deal with more and more patients. Senior staffs usually
understand such risk and educate the junior staffs on the subject. Risk assessment is
vital because it is a fundamental principle which rarely gets the attention it deserves.

50
0
103
50
37
05
101520253035404550
Percents (%)
Respond
Awareness of the risk exposed to others (e.g. public)
Strongly DisagreeDisagreeNeitherAgreeStrongly Agree
Figure 4.22: Awareness of the risk exposed to others (e.g. public)
The next question touches on the management plan outlined by the hospital.
The purpose of this question is to determine their familiarity with the plan.
Approximately 64% of the respondents either strongly agree or agree that they are
familiar with the management plan. Quite a substantial amount of the respondents are
either disagree or neither one with the statement. It is vital that the hospital
administration brief the healthcare staffs on the management plan.
3
2013
47
17
0
10
20
30
40
50
Percents (%)
Respond
Familiarity of the respondents towards the management plan
Strongly DisagreeDisagreeNeitherAgreeStrongly Agree
Figure 4.23: Familiarity of respondents towards the management plan

51
The seventh scaled question tests the respondents on their ability to identify
various types of clinical wastes. 64% of the respondents either strongly agree or agree
that they have the ability to identify various types of clinical wastes. However 36% of
the respondents either disagree or answer neither to the question. This proves to be
alarming as the ability to identify various types of clinical wastes is important in the
segregation process.
Ability of the respondents to identify types of clinical wastes
0% 10%
26%
51%
13%Strongly DisagreeDisagreeNeitherAgreeStrongly Agree
Figure 4.24: Ability of the respondents to identify types of clinical wastes
The next question is interrelated with the previous one which gauges the
ability of identification. The processes after the identification are segregation,
containment and labelling. The question will gauge the respondent’s ability to
perform the aforementioned processes. 17 % of the them strongly disagree and 43%
of them agree that they possess the ability to perform the tasks mentioned above. The
ability to perform the tasks is gained through work experience dealing with the
clinical wastes.

52
Ability of respondents to segregate, contain and label the clinical wastes
320
13
43
17
Strongly Disagree Disagree Neither Agree Strongly Agree
Figure 4.25: Ability of respondents to segregate, contain and label the clinical wastes
The next question is on one of the elements of clinical waste management
system which is the storage facility. When approached by the question that enquires
about their awareness of the storage facility, 17% of them strongly disagree and 57%
of them agree with the statement. Though they need not to be concerned with storage
facility as the concessionaire (Radicare Sdn Bhd) takes the full responsibility to
operate the storage, they should be aware of the location of the storage area.
Awareness of the respondents towards the storage facility
0
20
7
57
17
0
10
20
30
40
50
60
Respond
Perc
ents
(%)
Strongly Diagree Disagree Neither Agree Strongly Agree
Figure 4.26: Awareness of the respondents towards the storage facility

53
Record keeping is seldom given the much attention it deserves. When the
respondents are asked by the question, there are 40% of them who neither agree nor
disagree that they are aware of record keeping. Though record keeping is insignificant
if compared to identification, segregation or storage, it is vital in keeping track of the
flow of the clinical wastes from the point of generation to disposal. Manifest system
is implemented to ensure that cradle to grave principle of handling hazardous waste is
successful.
Awareness of the respondents to record keeping
17
40
30
13
0
510
15
2025
30
3540
45
Respond
Perc
ents
(%) Strongly Disagree
DisagreeNeitherAgreeStrongly Agree
Figure 4.27: Awareness of the respondents to record keeping
The last question of the second part of the survey is related to environment.
Clinical waste should not be under any circumstances be exposed to the environment
as it will destruct the natural habitat of the organisms. 84% of the respondents either
strongly agree or agree with the statement that clinical wastes will have significant
environmental impacts if they are not handled properly.

54
Awareness of the effects of clinical wastes to the environment
0
107
57
27
0
10
20
30
40
50
60
Respond
Perc
ents
(%)
Strongly Disagree Disagree Neither Agree Strongly Agree
Figure 4.28: Awareness of the effects of clinical wastes to the environment
Generally, from the analysis of the scaled questions, it is deduced that the
management components are well in place as the result of effective cooperation
between Hospital Tengku Ampuan Rahimah and Radicare (M) Sdn Bhd. However
there are some fields that need attention such as record keeping. Many of the staffs do
not realise that their day to day work dealing with clinical wastes involve some form
of record keeping. The awareness towards the effects of clinical wastes on
environment if improperly handled is strong as indicated by the figure 4.16 above.

55
CHAPTER V
CONCLUSIONS AND RECOMMENDATIONS
5.1 Latest development of clinical waste generation
According to the latest statistics released by Hospital Tengku Ampuan
Rahimah, Klang, the amount of the patients who visit the hospital has increased over
the years. Affordability of the healthcare services prepared by the hospital is one of
the driving forces behind the surge. This hospital not only caters to the need of the
district of Klang but also other districts. Hospitals from other districts often refer their
patients to the specialist services in HTAR. The increase of patients translate into
greater amount of clinical waste being generated.
Figure 5.1: The amount of patients admitted to the emergency ward

56
From the graph above, the amount of patients admitted to the emergency ward
increase from year to year. The increment will increase the workload of the healthcare
staffs, thus more people are needed to be recruited to meet the capacity.
Figure 5.2: The rate of bed usage in the hospital
It is easy to deduce from the graph above that the increasing rate of bed
usage among the patients of HTAR. With the rising number of patients, the clinical
wastes generated will increase at the same time. It is vital that the management
system can cope with the rising needs of patients.
Figure 5.3: The rate of bed capacity being empty from 2001-2005

57
The figure above shows a graph that represents the rate of bed being emptied.
The decreasing rate means that the bed capacity of HTAR being full at all time. This
development is caused by the increasingly affordability of government hospital
service
Figure 5.4: The rate of birth in HTAR from 2001 to 2005
Figure 5.5: Admission of patients to specialist clinic in HTAR from 2001 to 2004

58
5.2 Conclusions
Based on the observation made during the site visits, the clinical waste
management system adopted by Hospital Tengku Ampuan Rahimah, Klang is
effective and efficient. Close cooperation between the hospital and the concessionaire
appointed which is Radicare Sdn Bhd has worked greatly in management system.
Though the hospital only takes part in the segregation and containment of clinical
wastes, the responsibility is tremendous as improper segregation will cause disastrous
consequences. Identification and segregation which are done by the healthcare staffs
are observed to be adhering to the guidelines imposed by Radicare Sdn Bhd. From a
few inspections into the bins, the correct types of clinical wastes are being disposed
into the right bin. The subsequent processes which are packaging and labelling are
being carried out by the healthcare staffs.
Internal transportation will then be executed by the porters sent by Radicare
Sdn Bhd. The porters will push a wheeled bin to collect clinical wastes from every
ward and department. From casual observation, every porter is equipped with self
protection gear. Storage area which is operated under the supervision of RMSB is
well maintained. The absence of a cold storage facility means that the clinical wastes
stored need to be cleared out everyday. The external transportation is responsible of
moving the wastes to the incineration plant at Tanjung Panglima Garang, Banting.
Besides a site visit, a survey is carried out to gauge the awareness among the
healthcare staffs such as doctors and nurses towards the clinical waste management
system as executed by HTAR. From the response generated during the survey, the
awareness is considerably outstanding based on the analysis. The sample group of 30
people has given an average scale of 3.78 on the second part of the survey which is a
set of scaled questions. The group has responded remarkably well towards the
questions regarding to the components of management system. The majority of the
respondents have the knowledge and skill of dealing with clinical wastes. However,
some components such as record keeping need fine tuning as the responds are poor if
compared to the rest of the items surveyed.

59
5.3 Recommendations
The waste management strategy applied at the hospital was observed and
problematic areas were determined. All stages of waste management need
improvement, which mainly were due to human factor. In order too overcome these
obstacles the following actions were proposed for each stage of waste management.
It should be noted that environmental concern and pollution prevention are top
priority for the hospital. [10]
For the segregation components, proper training should be provided to
everyone involved in the waste management process regarding appropriate
segregation practices and the potential hazards associated with improper segregation.
It is vital to segregate the municipal wastes from the clinical wastes so as to reduce
the wastage of cost and manpower from the inconvenience caused by the improper
segregation.
For the packaging phase, purchase of good quality storage units that can
provide impermeability and resistance to perforation, and also be easy to handle and
clean. All bags should be labelled with the name of the department where they are
produced, as well as the collection date. The biological hazard symbol must be
printed on bags used to collect infectious or other hazardous wastes.
During the transport phase, purchase of good quality carts that would provide
impermeability, be resistant to perforation, and also be easy to handle and clean. The
carts must be labelled with the name of the department in which they are used. Last
and not least, for storage purposes it is important to impose strict entrance
prohibition into waste storerooms. It is important to adjust the frequency of waste
collection according to the facility’s waste production. Wastes should not remain in
any storeroom for more than 24 hours. It is strongly suggested to introduce e-
manifest system to improve the documentation of the movement of clinical
wastes.[11]

60
5.4 Further studies
The clinical waste management falls under the scope of hazardous waste
management. A further study on this topic is suggested on the incineration and the air
pollution control measures to avoid the contamination from the incinerator from
being exposed to the environment. A study on the awareness of the public towards
the clinical waste management also can be carried out. The awareness level may vary
from person to person depending on the education background.
The companies being appointed by Department of Environment are different
from region to region. Tongkah Medivest Sdn Bhd is appointed to southern region,
Radicare (M) Sdn Bhd is for the middle region while Fabel Mediserve Sdn Bhd is for
the northern region and east Malaysia. A study is suggested to compare the three
different companies. Further study can be carried out to compare the management
system of a government hospital and private hospital.

61
REFERENCES
1. Wayne L. Turnberg (1996). Biohazardous Waste : Risk Assessment, Policy,
and Management. John Wiley & Sons Inc.
2. Peter A. Reinhardt, Judith G. Gordon (1991). Infectious and Medical Waste
Management. Lewis Publishers
3. U.S. Environmental Protection Agency (1991). Medical Waste Management
and Disposal. Noyes Data Corporation
4. C.H. Collins (1991). Treatment and disposal of clinical and laboratory waste.
Medical Laboratory Sciences.
5. Patrick Lavelle (1998). How Hazardous Is Hospital Waste? World Wastes.
6. J.I Blenkharn (2005). Medical waste management in the south of Brazil.
Waste Management.
7. A. Bdour, B. Altrabsheh, N. Hadadin, M. Al-Shareif (2006). Assessment of
medical waste management processes: A case study of the northern part of
Jordan. Waste Management
8. M. Tsakona, E. Anagnostopoulou, E. Gidarakos (2006). Hospital waste
management and toxicity evaluation: A case study. Waste Management
62
9. Dr Leela Anthony (2006). Potential risks and hazards of not implementing a
proper clinical waste management system. Waste Management Conference
and Exhibition 2006.
11. Camille Martin (2006). Best Management Practices for Hospital Wastes.
Hospital and Clinical Wastes Reduction and Management Conference.
12. Office of Solid Waste RCRA Hazardous Waste (2004). e-Manifest Roadmap
conference proceedings. US Environmental Protection Agency
13. Zamastura Binti Ibrahim (2005). Management and Disposal of Clinical
Waste (Case Study: Hospital Kebangasaan Malaysia). Universiti Teknologi
Malaysia

63
Appendix A: Questionnaire form
1. Please state your gender? Male Female 2. Please state your age
<20 20 – 30 30-40 40-50 >50
3. Have you ever been involved in any accident involving clinical wastes? Yes No 4. How many years have you been working in the hospital? <10 10 - 15 15 - 20 20 - 25 25 - 30 > 30
5. What do you work as in the hospital? Doctor Nurse Administrator Others Please State:
64
Please tick on the box that best represents you.
Strongly Disagree Disagree Neither Agree
Strongly Agree
1. I have the knowledge of the definition of clinical waste
2. My training is sufficient to deal with any accident with clinical waste spills
3. Clinical waste management follows the standard procedure
4. I am aware of danger exposed to myself by the clinical wastes
5. I am aware of the danger exposed to others by the clinical wastes
6. I am familiar with the clinical waste management plan by the hospital
7. I am able to identify various type of clinical wastes
8. I know how to segregate, contain and label the clinical wastes properly
9. I know the location of the storage area of the clinical wastes
10. Record keeping of the clinical wastes is done properly
11. I am aware of the effects of the clinical wastes to the environment.

65
Appendix B: Clinical Waste Record Sheet

66
Appendix C: Clinical Waste Transportation Documentation