kementerian kesihatan...
TRANSCRIPT
KEMENTERIAN KESIHATAN MALAYSIA
0
MANUAL PELAKSANAAN
PROGRAM JAMINAN MUTU (QAP)
DALAM PERKHIDMATAN
PERUBATAN NUKLEAR
Dikemaskini oleh,
Kumpulan Kerja Program Jaminan Mutu Dalam Perkhidmatan Perubatan Nuklear Di
Bawah Akta Perlesenan Tenaga Atom 1984 (Akta 304)
Kementerian Kesihatan Malaysia
Mac 2016 (Edisi 2)
KEMENTERIAN KESIHATAN MALAYSIA
1
1. PENGENALAN
Program Jaminan Mutu (Quality Assurance Programme, QAP) di Kementerian
Kesihatan Malaysia telah dilancarkan pada tahun 1985. Objektif pelaksanaan QAP
adalah untuk memastikan pelanggan mendapat faedah daripada perkhidmatan yang
disediakan pada tahap yang optimum dengan sumber yang sedia ada. Indikator-
indikator diwujudkan untuk memantau kualiti pelbagai perkhidmatan dari aspek
penjagaan, pengurusan pelanggan, penggunaan sumber dan kepuasan pelanggan.
Dalam konteks pelaksanaan QAP yang menggunakan sinaran mengion bagi tujuan
diagnosis dan terapi, kepentingan pesakit perlu diutamakan. Ini dapat dicapai
dengan dedahan dos sinaran yang tepat dan optimum di samping dedahan sinaran
kepada pekerja dan orang awam adalah terkawal. Manakala penggunaan punca
sinaran mengion terlibat akan sentiasa dipantau dari aspek keselamatan termasuk
sekuriti. Melalui langkah-langkah sebegini, diharap dapat mencapai objektif
pelaksanaan QAP secara menyeluruh dan berkesan.
Keperluan pelaksanaan QAP selaras dengan Peraturan 41.(d) & 41.(e) dalam
Peraturan-Peraturan Perlesenan Tenaga Atom (Perlindungan Sinaran Keselamatan
Asas) 2010 iaitu:
“41. Tiap-tiap pemegang lesen atau majikan hendaklah memastikan bahawa:
d) bagi penggunaan sinaran secara diagnostik, program Penjaminan mutu yang
dinyatakan oleh pihak berkuasa yang berkenaan dijalankan oleh atau di
bawah penyeliaan seorang pakar yang berkelayakan dalam fizik perubatan;
e) bagi penggunaan sinaran secara terapeutik termasuk teleterapi atau
brakiterapi, penentukuran, dosimetri dan program Penjaminan mutu yang
dinyatakan oleh pihak berkuasa yang berkenaan dijalankan oleh atau di
bawah penyeliaan seorang pakar yang berkelayakan dalam fizik perubatan;”
Selain itu, Peraturan
“53. (1) juga menyatakan bahawa sebagai tambahan kepada pemakaian kehendak
yang berkaitan bagi jaminan mutu, pemegang lesen hendaklah mewujudkan suatu
program jaminan mutu yang komprehensif bagi dedahan perubatan dengan
penglibatan pakar berkelayakan yang sesuai dalam bidang yang berkaitan
sebagaimana yang dinyatakan oleh pihak berkuasa yang berkenaan.”
Mesyuarat Jawatankuasa Penasihat Radiologi (RAC) ke-37 yang diadakan pada
15hb Julai 2010 telah memutuskan supaya pelaksanaan QAP dalam perubatan
KEMENTERIAN KESIHATAN MALAYSIA
2
nuklear ke atas pusat perubatan nuklear kerajaan dan swasta diwujudkan. Melalui
pelaksanaan QAP tersebut, diharapkan pusat-pusat perubatan nuklear akan dapat
menerap dan mengamalkan budaya kualiti dan selamat dalam penggunaan sinaran
mengion untuk tujuan perubatan kepada pesakit, pekerja dan orang awam.
Untuk memastikan QAP dilaksanakan dengan berkesan, jabatan berkaitan perlu
mewujudkan kumpulan staf yang sekurang-kurangnya terdiri daripada seorang
Pakar Perubatan Nuklear, Ahli Fizik Perubatan, Ahli Farmasi (Nuklear),
Juruteknologi Perubatan Nuklear dan lain-lain profesion yang terlibat.
2. OBJEKTIF
Objektif pelaksanaan QAP dalam perkhidmatan perubatan nuklear adalah:
2.1 Mempertingkatkan kualiti perkhidmatan dalam perubatan nuklear.
2.2 Memastikan penghasilan maklumat klinikal yang diperlukan dengan
penggunaan radioaktiviti yang optimum.
2.3 Memastikan penggunaan sumber yang sedia ada secara efektif.
2.4 Memenuhi dan mematuhi keperluan regulatori di bawah Akta Perlesenan
Tenaga Atom 1984.
3. SKOP
Skop Jaminan Mutu bagi perkhidmatan perubatan nuklear merangkumi komponen-
komponen seperti berikut:
(a) Sejarah klinikal pesakit
Prosedur diperlukan bagi membolehkan maklumat sejarah pesakit dapat
diketahui sebelum perancangan rawatan dapat dikenalpasti.
Contohnya maklumat sejarah klinikal pesakit, soalan-soalan klinikal,
kesesuaian pemeriksaan dan kontraindikasi.
(b) Perancangan prosedur
Perancangan prosedur perlu dilaksanakan untuk memastikan pesakit
mendapat rawatan yang bertepatan dengan jenis penyakit bagi
mengelakkan kesilapan dalam pemberian dos kepada pesakit.
Ini merangkumi kebolehpercayaan prosedur pentadbiran (reliable
administrative procedures), maklumat pesakit serta prosedur persediaan
pesakit.
KEMENTERIAN KESIHATAN MALAYSIA
3
(c) Prosedur klinikal
Prosedur klinikal perlu dilaksanakan untuk memastikan rawatan yang
diberikan adalah tepat dan mematuhi prinsip perlindungan sinaran serta
segala aktiviti yang berkaitan dengan pengurusan bahan radioaktif
dikendalikan secara selamat dan terkawal.
Prosedur klinikal perlu mengambilkira perkara-perkara seperti pembekal dan
bahan radioaktif yang diluluskan, penyimpanan bahan radioaktif, persediaan,
persekitaran klinikal, pengurusan dan persediaan pesakit, prestasi radas,
protokol pengendalian, pelupusan sisa radioaktif, pergerakan bahan
radioaktif.
(d) Latihan dan pengalaman
Semua personel yang terlibat seperti Pakar Perubatan Nuklear, Ahli Fizik
Perubatan, Ahli Farmasi (Nuklear), Juruteknologi Perubatan Nuklear dan
lain-lain yang terlibat perlu mempunyai latihan dan pengalaman yang sesuai.
(e) Penganalisaan data
Data-data yang diperolehi semasa prosedur pengimejan adalah sangat
penting untuk membekalkan maklumat diagnosis yang tepat. Ini dipengaruhi
oleh protokol pemprosesan data, prestasi peralatan, ketepatan dan integriti
data yang diperolehi.
(f) Laporan
Laporan diagnosis dan rawatan yang disediakan merangkumi data,
penyemakan semula imej, keputusan dan nasihat lanjutan oleh Pakar
Perubatan Nuklear bagi memastikan perkhidmatan perubatan nuklear yang
berkualiti.
(g) Hasil perkhidmatan (general outcomes)
Pelaksanaan QAP yang berkesan dapat ditentukan melalui keberhasilan
klinikal (clinical outcome), dos dedahan radiasi, kepuasan pesakit serta
kepuasan doktor/pakar yang merujuk.
(h) Audit
Proses audit adalah penting dalam pelaksanaan QAP bagi memastikan
kelemahan/ketidakpatuhan yang berlaku dapat diambil tindakan pencegahan
dan penambahbaikan bagi meningkatkan kualiti perkhidmatan yang
diberikan.
KEMENTERIAN KESIHATAN MALAYSIA
4
4. PELAKSANAAN QAP DI BAWAH AKTA 304
Pelaksanaan QAP hendaklah merangkumi elemen-elemen yang diwajibkan seperti di
bawah:
4.1 INDIKATOR – KADAR KAJIAN BERULANG (RATE OF REPEAT STUDIES)
Pemonitoran dan analisa kajian kes berulang hendaklah diwujudkan di setiap
pusat perubatan nuklear. Laporan pemonitoran dan analisa termasuk tindakan
pembaikan yang telah diambil perlu dikaji setiap tahun. Kadar kajian kes berulang
hendaklah tidak melebihi 5%. Maklumat lanjut mengenai indikator adalah seperti
di Lampiran A1 dan Lampiran A2.
4.2 KAWALAN MUTU (QC) PERALATAN PENGIMEJAN DAN KEMUDAHAN
BERKAITAN
Semua peralatan pengimejan dan kemudahan berkaitan di pusat perubatan
nuklear hendaklah menjalani ujian kawalan mutu (QC) bagi memastikan
pematuhan terhadap piawaian dan prestasi yang ditetapkan. Pelaksanaan QC
bagi peralatan pengimejan dan kemudahan berkaitan perlu merangkumi ujian
penerimaan (acceptance tests) dan ujian kawalan mutu secara berkala. Ujian
penerimaan on site perlu dijalankan bersama pengilang/pembekal setelah
peralatan dipasang. Selain memastikan prestasi peralatan memenuhi spesifikasi
pengilang yang ditetapkan, ujian penerimaan perlu dilakukan bagi mendapatkan
data rujukan (baseline data).
Ujian QC bagi semua peralatan pengimejan dan kemudahan berkaitan hendaklah
dilaksanakan secara berkala mengikut tempoh yang ditetapkan bagi mematuhi
keperluan piawaian prestasi dan keselamatan seperti dalam Lampiran B.
Pengujian ini juga perlu dijalankan selepas kerja-kerja pembaikan atau
pertukaran sebarang komponen peralatan yang boleh menjejaskan fungsi dan
prestasi peralatan atau kemudahan berkaitan. Di samping itu, peralatan
pengukuran sinaran hendaklah dipastikan ditentukur secara berkala.
Kerja-kerja pembaikan perlu dijalankan sekiranya prestasi peralatan pengimejan
dan kemudahan berkaitan tidak mematuhi spesifikasi atau/dan piawaian yang
ditetapkan. Pengujian penerimaan dan QC hendaklah dijalankan dan disahkan
oleh personel yang diiktiraf oleh pihak berkuasa KKM.
KEMENTERIAN KESIHATAN MALAYSIA
5
4.3 PENDIDIKAN PERUBATAN SECARA BERTERUSAN (CME)
Semua personel hendaklah menghadiri program pendidikan perubatan secara
berterusan yang diiktiraf oleh pihak berkuasa di bawah Akta 304 untuk
meningkatkan pengetahuan dan kompetensi mereka. Tempoh latihan hendaklah
sekurang-kurangnya 6 jam terkumpul setahun dengan merangkumi sekurang-
kurangnya 3 bidang seperti berikut:
Radiation Safety Awareness in Nuclear Medicine
Accident and Emergency Preparedness
Update in Nuclear Medicine Technologies
Update in Radiopharmaceutical
Clinical Procedures/Protocol Update
Image/Fusion Image Reporting
Management of Quality Assurance Program
Legislation and Regulatory Requirement
Bukti kehadiran kursus seperti sijil/senarai kehadiran yang disahkan oleh
penganjur/ketua jabatan hendaklah direkod dan dikemukakan kepada pihak
berkuasa KKM.
5. PENGURUSAN REKOD
Rekod-rekod berkaitan dengan kawalan mutu (QC), indikator, CME dan lain-lain
yang berkaitan hendaklah diurus dan disimpan mengikut tempoh yang ditetapkan
oleh pihak berkuasa KKM.
KEMENTERIAN KESIHATAN MALAYSIA
6
6. DEFINISI
Dalam manual ini, melainkan jika konteksnya menghendaki makna yang lain:
Ahli Farmasi (Nuklear)
Seseorang ahli farmasi berdaftar yang telah menjalani program latihan dalam bidang farmasi nuklear yang diluluskan oleh pihak berkuasa berkaitan. Juga digelar sebagai Pegawai Farmasi (Nuklear).
Ahli Fizik
Perubatan
Seseorang yang mempunyai pengetahuan, latihan dan pengalaman untuk mengaplikasikan prinsip-prinsip fizik untuk tujuan diagnosis dan rawatan dalam bidang perubatan yang berkenaan. Juga digelar sebagai Pegawai Sains (Fizik).
Data rujukan Nilai atau keputusan yang diperolehi semasa ujian
penerimaan.
Fizik perubatan Bidang pengkhususan yang melibatkan penggunaan dan
pemakaian fizik dalam perubatan.
Indikator Sesuatu perkara yang telah dirancang, dipersetujui dan
dilaksanakan untuk mengenalpasti tahap kualiti bagi
perkhidmatan yang diberi. Juga dikenali sebagai quality
indicator.
Juruteknologi
Perubatan Nuklear
Seseorang personel kesihatan bersekutu berdaftar yang telah
menerima latihan khas dalam bidang perubatan nuklear yang
diluluskan oleh pihak berkuasa berkenaan. Personel ini
bertanggungjawab dalam menjalankan tugas pengimejan
perubatan nuklear dan ujian in-vitro yang melibatkan
pengukuran sinaran serta memberi (administer)
radiofarmaseutikal kepada pesakit untuk tujuan diagnosis di
bawah pemantauan Pakar Perubatan Nuklear.
Pakar Perubatan
Nuklear
Seseorang pengamal perubatan berdaftar yang telah
menerima latihan khas dalam perubatan nuklear yang
diluluskan oleh pihak berkuasa berkenaan dan mempunyai
pengetahuan khas mengenai penggunaan radiofarmaseutikal
atau radionuklid untuk prosedur diagnosis dan rawatan.
KEMENTERIAN KESIHATAN MALAYSIA
7
Perubatan nuklear Bidang pengkhususan perubatan yang melibatkan semua
pemakaian bahan radioaktif dalam diagnosis atau rawatan
atau dalam penyelidikan perubatan kecuali penggunaan
punca terkedap dalam radioterapi.
Program Jaminan
Mutu
Pengurusan dan prosedur keseluruhan yang merangkumi
tindakan penjaminan mutu untuk pelaksanaan perkhidmatan
perubatan nuklear. Ia merupakan suatu aktiviti terancang
untuk memberi penjaminan mutu dalam perkhidmatan yang
melibatkan teknik kawalan mutu dan prosedur pentadbiran
berkualiti. Komponen dan tahap pelaksanaan aktiviti ini
adalah bergantung kepada jenis dan saiz kemudahan, jenis
prosedur yang dilakukan dan faktor lain-lain yang berkaitan.
Radiofarmaseutikal Bahan radioaktif atau produk termasuk sebatian tidak organik
dan organik, peptide, protein, monoklonal antibodi, fragment
dan oligonucleotide yang dilabel dengan radionuklid yang
mempunyai separuh hayat dari beberapa saat hingga
beberapa hari untuk tujuan diagnostik dan kegunaan
terapeutik.
Ujian penerimaan Ujian bagi mengenalpasti sesuatu radas yang diterima adalah
mengikut spesifikasi teknikal yang dipersetujui dan nilai
keputusan ujian-ujian ini akan menjadi nilai rujukan kepada
ujian berkala yang dijalankan pada masa hadapan.
7. SINGKATAN
CFOV Central Field of View
COR Center of Rotation
CME Continuous Medical Education
cps counts per second
CT Computed Tomography
FWHM
IAEA
Full Width at Half Maximum
International Atomic Energy Agency
kBq kiloBecquerel
KKM Kementerian Kesihatan Malaysia
PET Positron Emission Tomography
PHA Pulse Height Analyzer
KEMENTERIAN KESIHATAN MALAYSIA
8
QAP Quality Assurance Programme
QC Quality Control
RAC Radiological Advisory Committee
SPECT Single Photon Emission Computed Tomography
TR Tomography Resolution
UFOV Useful Field of View
8. RUJUKAN
i) Akta Perlesenan Tenaga Atom 1984 (Akta 304).
ii) Peraturan-Peraturan Perlesenan Tenaga Atom (Perlindungan Sinaran
Keselamatan Asas) 2010.
iii) Surat Pekeliling Ketua Pengarah Kesihatan Malaysia Bil. 26/2010: Keperluan
Pakar Perubatan Nuklear Bagi Perkhidmatan Perubatan Nuklear Di Bawah Akta
Perlesenan Tenaga Atom 1984 (Akta 304) Bagi Maksud Perubatan.
iv) IAEA Human Health Series No. 1: Quality Assurance for PET and PET/CT
Systems. Vienna: IAEA.
v) IAEA Human Health Series No. 6: Quality Assurance for SPECT Systems.
Vienna: IAEA.
vi) IAEA Safety Reports Series No. 4: Applying Radiation Safety Standards in
Nuclear Medicine. Vienna: IAEA.
vii) World Health Organization. Quality Assurance in Nuclear Medicine. Geneva:
WHO.
viii) Ministry of Health Malaysia. Quality Assurance-A Problem Solving Approach.
Kuala Lumpur: MOH.
ix) Family Health Development Division, Ministry of Health Malaysia. 2008. Quality
Assurance Programme Manual. Putrajaya: MOH.
x) H. Wengenmair, J. Kopp. Gamma Probes for Sentinel Lymph Node
Localization: Quality Criteria, Minimal Requirements and Quality of
Commercially Available Systems. Germany: Central Clinic, Augsburg.
xi) Operational Guidance on Hospital Radiopharmacy: A Safe and Effective
Approach, Vienna IAEA, 2008.
xii) Guides to the Development of Radiopharmaceutical Preparation Facilities for
Healthcare Establishments, 1st Edition, Pharmaceutical Services Division: MOH,
2010.
xiii) G.B. Saha. Fundamentals of Nuclear Pharmacy, 6th Edition, SpringerVerlag,
New York.
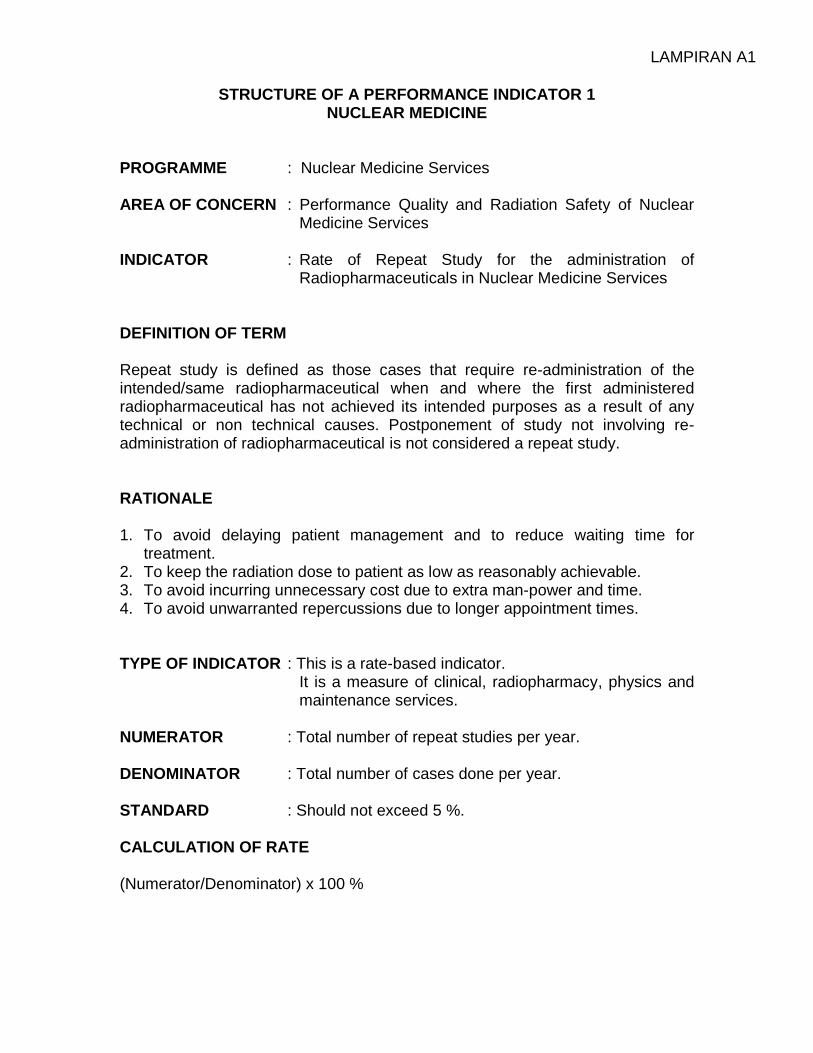
LAMPIRAN A1
STRUCTURE OF A PERFORMANCE INDICATOR 1
NUCLEAR MEDICINE PROGRAMME : Nuclear Medicine Services AREA OF CONCERN : Performance Quality and Radiation Safety of Nuclear
Medicine Services INDICATOR : Rate of Repeat Study for the administration of
Radiopharmaceuticals in Nuclear Medicine Services DEFINITION OF TERM Repeat study is defined as those cases that require re-administration of the intended/same radiopharmaceutical when and where the first administered radiopharmaceutical has not achieved its intended purposes as a result of any technical or non technical causes. Postponement of study not involving re-administration of radiopharmaceutical is not considered a repeat study. RATIONALE 1. To avoid delaying patient management and to reduce waiting time for
treatment. 2. To keep the radiation dose to patient as low as reasonably achievable. 3. To avoid incurring unnecessary cost due to extra man-power and time. 4. To avoid unwarranted repercussions due to longer appointment times. TYPE OF INDICATOR : This is a rate-based indicator.
It is a measure of clinical, radiopharmacy, physics and maintenance services.
NUMERATOR : Total number of repeat studies per year.
DENOMINATOR : Total number of cases done per year. STANDARD : Should not exceed 5 %. CALCULATION OF RATE (Numerator/Denominator) x 100 %
LAMPIRAN A1
EXPLANATION Rate of Repeat Studies
– This is a clinical audit to look into the quality of performance after an imaging study.
– It is based on the basis that if the required clinical information can be obtained
from a study, there is no need to repeat it. Definition of repeat study 1. Any failed study after administration of radiopharmaceutical where there is no
information available or any study that needs to be repeated due to inadequate information that require administration of the intended/same radiopharmaceutical whether on the same day (e.g. Technetium thyroid scan) or on a different day (e.g. Renal DTPA study).
2. The following would not be considered as a repeat study:
a. Quantitative reanalysis of studies
As the study data is still available on computer
b. Reprinting of Scan ordered by doctor
c. Studies not performed because of equipment or radiopharmaceutical problems
3. Reasons for a repeat study:
a. Human factors (i) Staff – administration problems
failed administration or extravasation of radiopharmaceutical
incorrect radiopharmaceuticals administration – image acquisition problems
incorrect field, inadequate counts obtained, inadequate views obtained
– computer problems
accidental deletion of patient studies (ii) Patient – motion artefacts due to:
inadequate instructions to patient
inadequate sedation, especially in children
uncooperative child – case cancellations due to unstable patient
b. Machine factors
– Intrinsic problems in gamma camera or power interruptions – Computer problems (crashes) – Contamination on the machine
LAMPIRAN A1
c. Radiopharmaceutical factors – Faulty radiopharmaceutical (undetected by QC) – Incorrect QC procedure – Inadequate dose of radiopharmaceutical which lead to poor quality
image – Drug Interactions
(b) and (c) should normally be addressed through proper QC measures. Methodology 1. Data Collection Any repeat study must be recorded immediately in a record book reserved for this purpose and signed by the relevant staff. The responsible person/licensee or the delegated staff should ensure the Form A1 is completed before the end of the day. 2. Data Analysis Data should be transferred from Form A1 to Form B1. Data analysis should be carried out by the responsible person/licensee or the delegated staff at least 3 monthly. An example of the final presentation format is in Appendix 1. Parameters may vary from time to time. Periodic trend analysis is recommended. 3. Action plan The root cause of each repeat study should be identified. Corrective and preventive measures should then be taken. 4. Annual Report Analysis of root cause identification and remedial action must be stated in the annual report. This annual report should be submitted to the appropriate authority yearly.
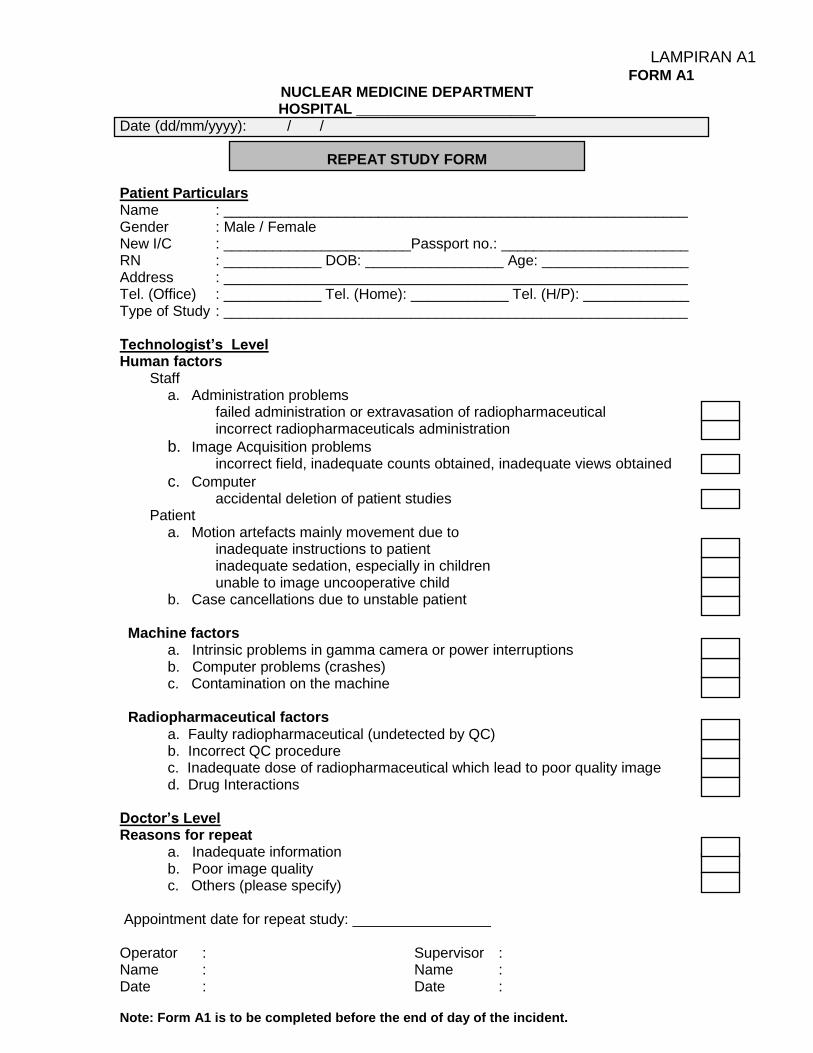
LAMPIRAN A1 FORM A1
NUCLEAR MEDICINE DEPARTMENT HOSPITAL ______________________
Date (dd/mm/yyyy): / /
REPEAT STUDY FORM Patient Particulars Name : _________________________________________________________ Gender : Male / Female New I/C : _______________________Passport no.: _______________________ RN : ____________ DOB: _________________ Age: __________________ Address : _________________________________________________________ Tel. (Office) : ____________ Tel. (Home): ____________ Tel. (H/P): _____________ Type of Study : _________________________________________________________ Technologist’s Level Human factors
Staff a. Administration problems
failed administration or extravasation of radiopharmaceutical incorrect radiopharmaceuticals administration
b. Image Acquisition problems incorrect field, inadequate counts obtained, inadequate views obtained
c. Computer accidental deletion of patient studies
Patient a. Motion artefacts mainly movement due to
inadequate instructions to patient inadequate sedation, especially in children unable to image uncooperative child
b. Case cancellations due to unstable patient Machine factors
a. Intrinsic problems in gamma camera or power interruptions b. Computer problems (crashes) c. Contamination on the machine
Radiopharmaceutical factors
a. Faulty radiopharmaceutical (undetected by QC) b. Incorrect QC procedure c. Inadequate dose of radiopharmaceutical which lead to poor quality image d. Drug Interactions
Doctor’s Level Reasons for repeat
a. Inadequate information b. Poor image quality c. Others (please specify)
Appointment date for repeat study: _________________ Operator : Supervisor : Name : Name : Date : Date : Note: Form A1 is to be completed before the end of day of the incident.
LAMPIRAN A1
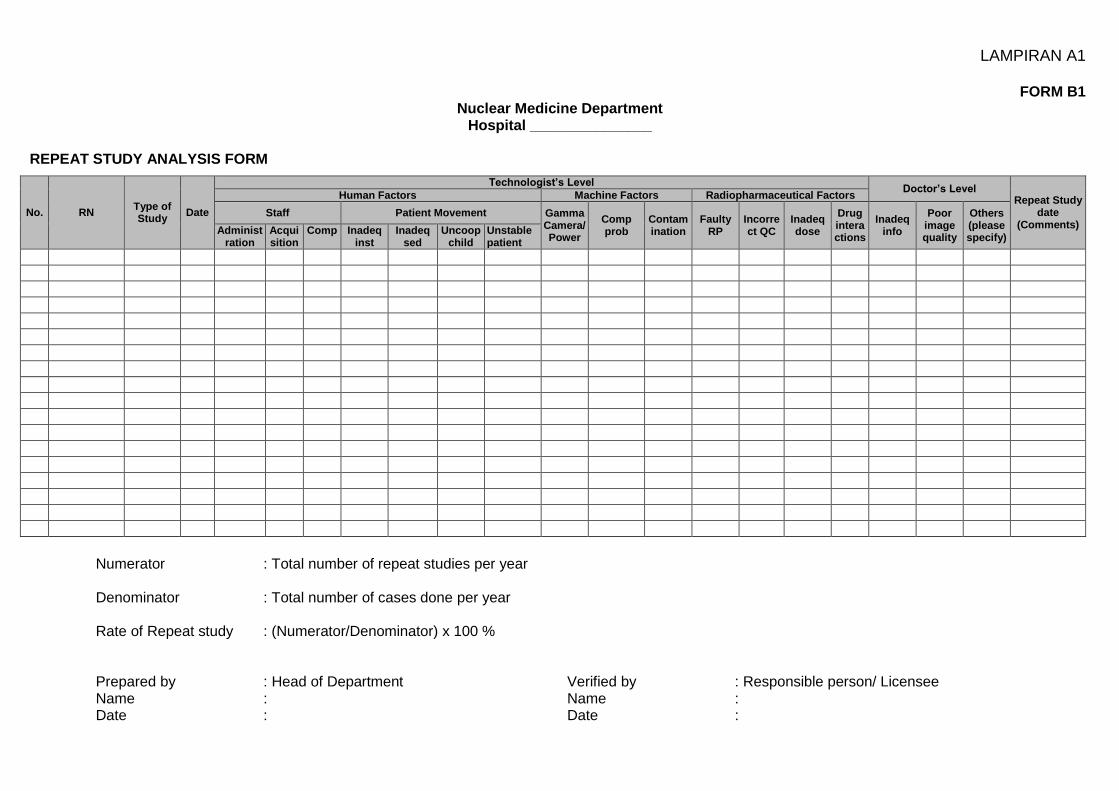
FORM B1 Nuclear Medicine Department
Hospital _______________
REPEAT STUDY ANALYSIS FORM
No. RN Type of Study
Date
Technologist’s Level Doctor’s Level
Repeat Study date
(Comments)
Human Factors Machine Factors Radiopharmaceutical Factors
Staff Patient Movement Gamma Camera/ Power
Comp prob
Contamination
Faulty RP
Incorrect QC
Inadeq dose
Drug interactions
Inadeq info
Poor image quality
Others (please specify)
Administration
Acquisition
Comp Inadeq inst
Inadeq sed
Uncoop child
Unstable patient
Numerator : Total number of repeat studies per year Denominator : Total number of cases done per year Rate of Repeat study : (Numerator/Denominator) x 100 % Prepared by : Head of Department Name : Date :
Verified by : Responsible person/ Licensee Name : Date :
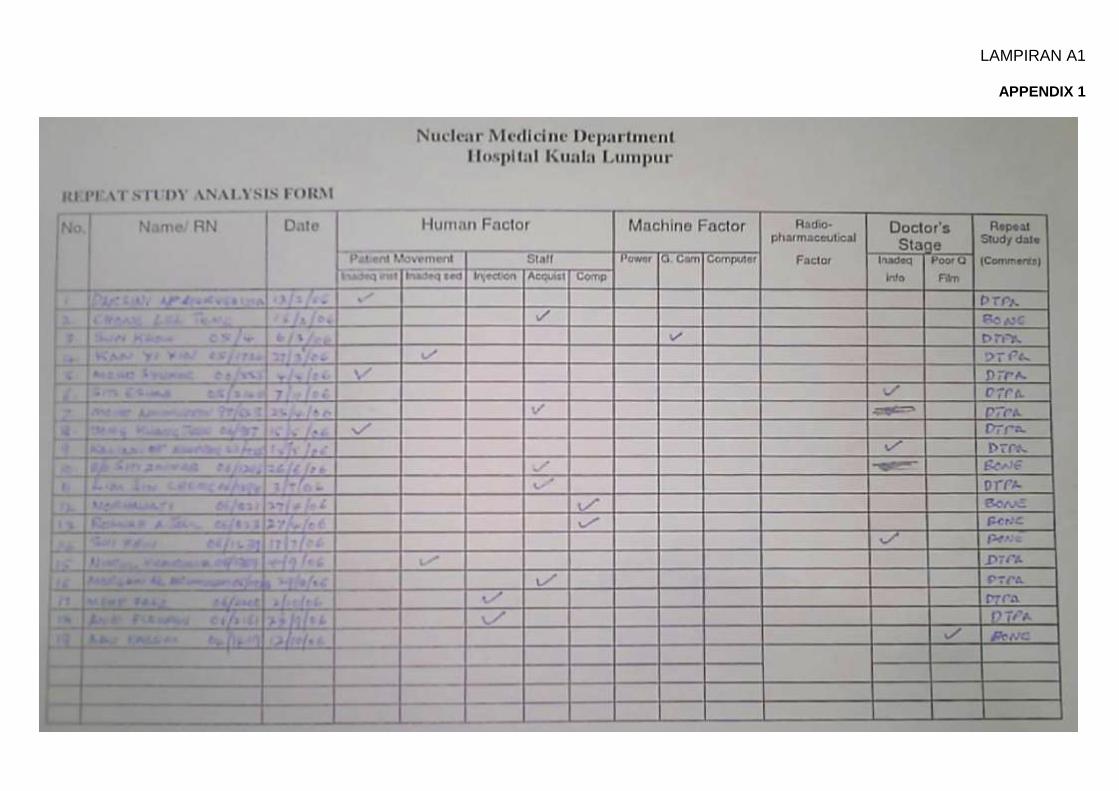
LAMPIRAN A1
APPENDIX 1
LAMPIRAN A2
STRUCTURE OF PERFORMANCE INDICATOR 2
NUCLEAR MEDICINE PROGRAMME : Nuclear Medicine Services AREA OF CONCERN : Performance Quality and Radiation Safety of Nuclear
Medicine Services INDICATOR : Rate of Repeat CT exposure for hybrid imaging in
Nuclear Medicine Services DEFINITION OF TERM Any repeat CT scan, be it partial or a full repeat study over the same region which has just been scanned, as the first CT acquisition has failed to achieve the initial intended purpose(s). The main purpose(s) for acquiring CT data in nuclear medicine hybrid imaging are for attenuation correction and/or anatomical correlation. RATIONALE Analysis of repeat CT exposure rate is a method effective in monitoring and reducing unnecessary radiation exposure to a patient. TYPE OF INDICATOR : This is a rate-based indicator. NUMERATOR : Total number of repeat CT exposure per year. DENOMINATOR : Total number of hybrid imaging cases (patients) done
per year. STANDARD : Should not exceed 5%. CALCULATION OF RATE (Numerator/Denominator) x 100 % EXPLANATION Rate of Repeat CT Exposure
1. This is a clinical audit to look into the rate of undesired, possibly avoidable CT radiation dose to the patients when hybrid imaging is used in nuclear medicine services.
2. Such situation arises when the initial acquired CT data has failed to provide satisfactory or adequate information for attenuation correction and/or anatomical correlation. As a result, a repeat scan (with or without the radionuclide imaging component) at the same site or part of the previously scanned site needs to be carried out in order to complete the study.
LAMPIRAN A2
3. The notion is based on the basis that should at all a proper planning and preparation have been carried out before the procedure, adequate CT data for that identified purpose(s) could have been attained in the first CT scan itself.
4. A sequential CT exposure carried out as part of the study protocol so as to be used for reporting will not be considered as a repeat CT exposure (example: (1) dual-time imaging protocol to ascertain benign inflammatory and malignant disease; (2) forced diuresis dual-phase bladder protocol for urinary bladder cancer or tumour at its close proximity).
5. The table below lists out some of the reasons for a repeat CT exposure:
Reasons for a repeat CT exposure
Human factors
a. Artefact (e.g. streaks, ring, jewellery or anything that could have been temporarily removed during imaging.)
b. Incorrect technical parameter (e.g. need higher mAs or some other technical adjustment etc.)
c. Incorrect positioning
d. Incorrect examination
e. Misregistration due to motion (including respiratory motion artefact)
f. Residual contrast (including oral contrast) left from previous radiological procedure
g. Failure or incorrect radiotracer injection resulting in a total repeat study
Machine factors
a. Scanner malfunction / down
b. Electrical power outage
Methodology
1. Data Collection
Any repeat CT exposure must be recorded immediately in a record book reserved for this purpose and signed by the relevant staff. The responsible person/licensee or the delegated staff should ensure the Form A2 is completed before the end of the day.
2. Data Analysis
Data should be transferred from Form A2 to Form B2. Data analysis should be carried out by the responsible person/licensee or the delegated staff to determine the reason for the repeat CT exposure, at least 3 monthly. Parameters may vary from time to time. Periodic trend analysis is recommended.
3. Action Plan
The root cause of each repeat CT exposure should be identified. Corrective and preventive measures should then be taken.
4. Annual Report
Analysis of root cause identification and remedial action must be stated in the annual report. This annual report should be submitted to the appropriate authority yearly.
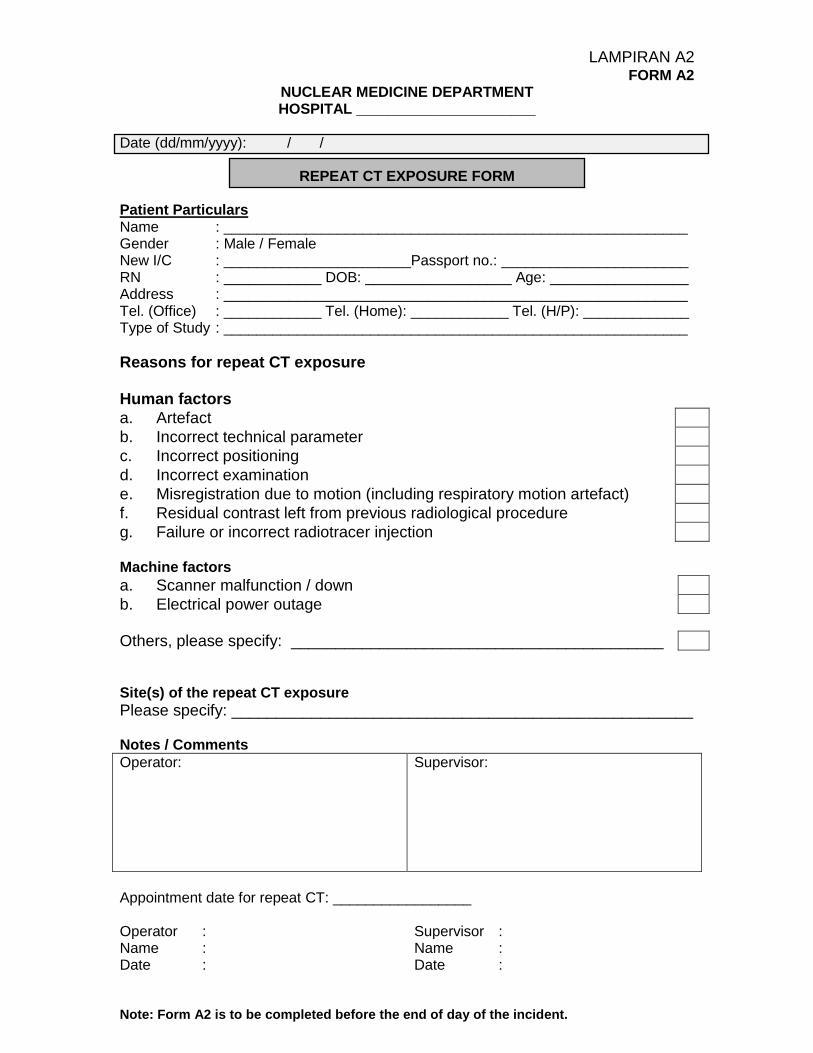
LAMPIRAN A2 FORM A2
NUCLEAR MEDICINE DEPARTMENT HOSPITAL ______________________
Date (dd/mm/yyyy): / /
REPEAT CT EXPOSURE FORM
Patient Particulars Name : _________________________________________________________ Gender : Male / Female New I/C : _______________________Passport no.: _______________________ RN : ____________ DOB: __________________ Age: _________________ Address : _________________________________________________________ Tel. (Office) : ____________ Tel. (Home): ____________ Tel. (H/P): _____________ Type of Study : _________________________________________________________
Reasons for repeat CT exposure Human factors
a. Artefact
b. Incorrect technical parameter
c. Incorrect positioning
d. Incorrect examination
e. Misregistration due to motion (including respiratory motion artefact)
f. Residual contrast left from previous radiological procedure
g. Failure or incorrect radiotracer injection Machine factors
a. Scanner malfunction / down
b. Electrical power outage
Others, please specify: __________________________________________ Site(s) of the repeat CT exposure
Please specify: ____________________________________________________ Notes / Comments
Operator:
Supervisor:
Appointment date for repeat CT: _________________ Operator : Supervisor : Name : Name : Date : Date : Note: Form A2 is to be completed before the end of day of the incident.
LAMPIRAN A2
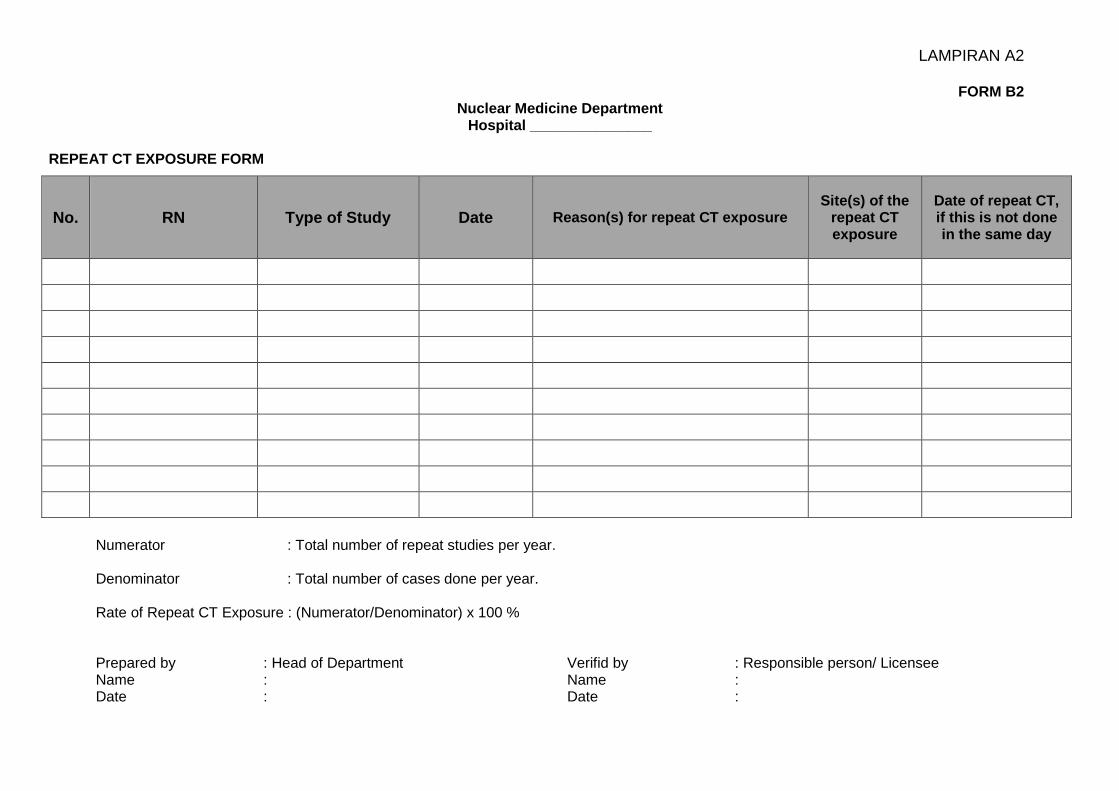
FORM B2 Nuclear Medicine Department
Hospital _______________
REPEAT CT EXPOSURE FORM
No. RN Type of Study Date Reason(s) for repeat CT exposure Site(s) of the
repeat CT exposure
Date of repeat CT, if this is not done in the same day
Numerator : Total number of repeat studies per year.
Denominator : Total number of cases done per year. Rate of Repeat CT Exposure : (Numerator/Denominator) x 100 % Prepared by : Head of Department Name : Date :
Verifid by : Responsible person/ Licensee Name : Date :
LAMPIRAN B
QUALITY CONTROL TESTS AND PERFORMANCE STANDARDS FOR EQUIPMENT USED IN NUCLEAR MEDICINE
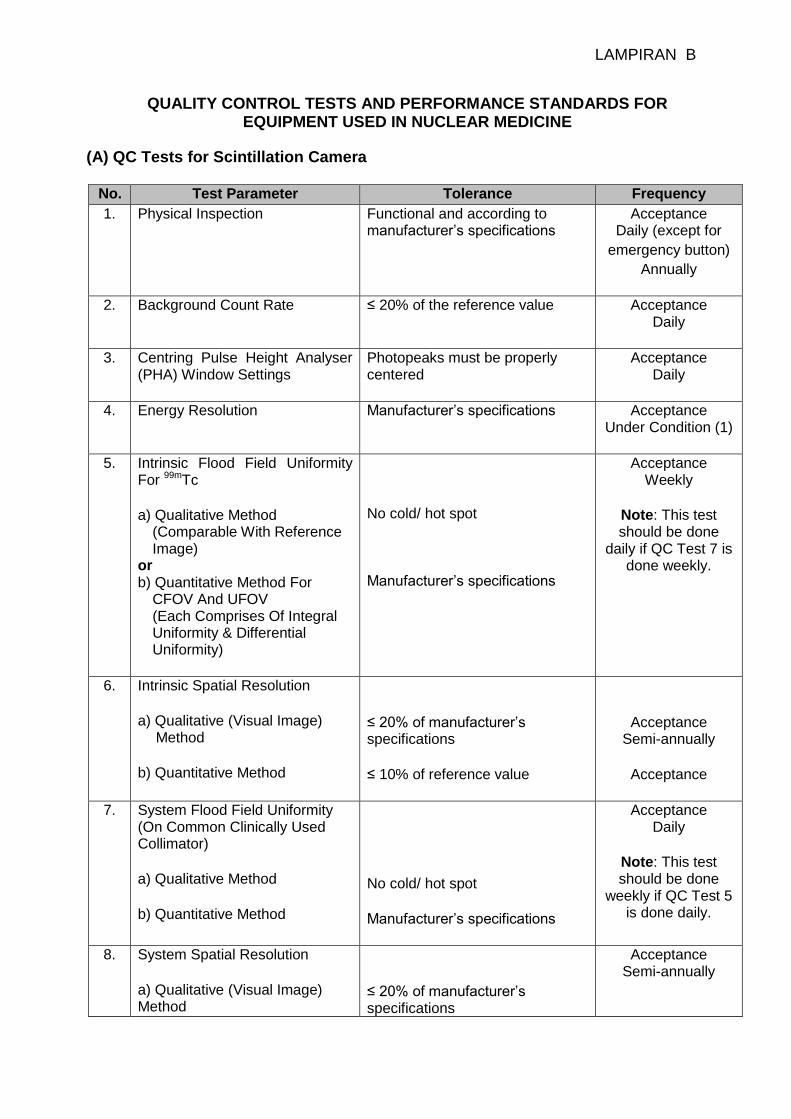
(A) QC Tests for Scintillation Camera No. Test Parameter Tolerance Frequency
1. Physical Inspection Functional and according to manufacturer’s specifications
Acceptance Daily (except for
emergency button)
Annually
2. Background Count Rate ≤ 20% of the reference value Acceptance Daily
3. Centring Pulse Height Analyser
(PHA) Window Settings
Photopeaks must be properly centered
Acceptance Daily
4. Energy Resolution Manufacturer’s specifications Acceptance Under Condition (1)
5. Intrinsic Flood Field Uniformity For 99mTc a) Qualitative Method
(Comparable With Reference Image)
or b) Quantitative Method For
CFOV And UFOV (Each Comprises Of Integral Uniformity & Differential Uniformity)
No cold/ hot spot Manufacturer’s specifications
Acceptance Weekly
Note: This test should be done
daily if QC Test 7 is done weekly.
6. Intrinsic Spatial Resolution a) Qualitative (Visual Image)
Method b) Quantitative Method
≤ 20% of manufacturer’s specifications ≤ 10% of reference value
Acceptance Semi-annually
Acceptance
7. System Flood Field Uniformity (On Common Clinically Used Collimator) a) Qualitative Method b) Quantitative Method
No cold/ hot spot Manufacturer’s specifications
Acceptance Daily
Note: This test should be done
weekly if QC Test 5 is done daily.
8. System Spatial Resolution a) Qualitative (Visual Image) Method
≤ 20% of manufacturer’s specifications
Acceptance Semi-annually
LAMPIRAN B
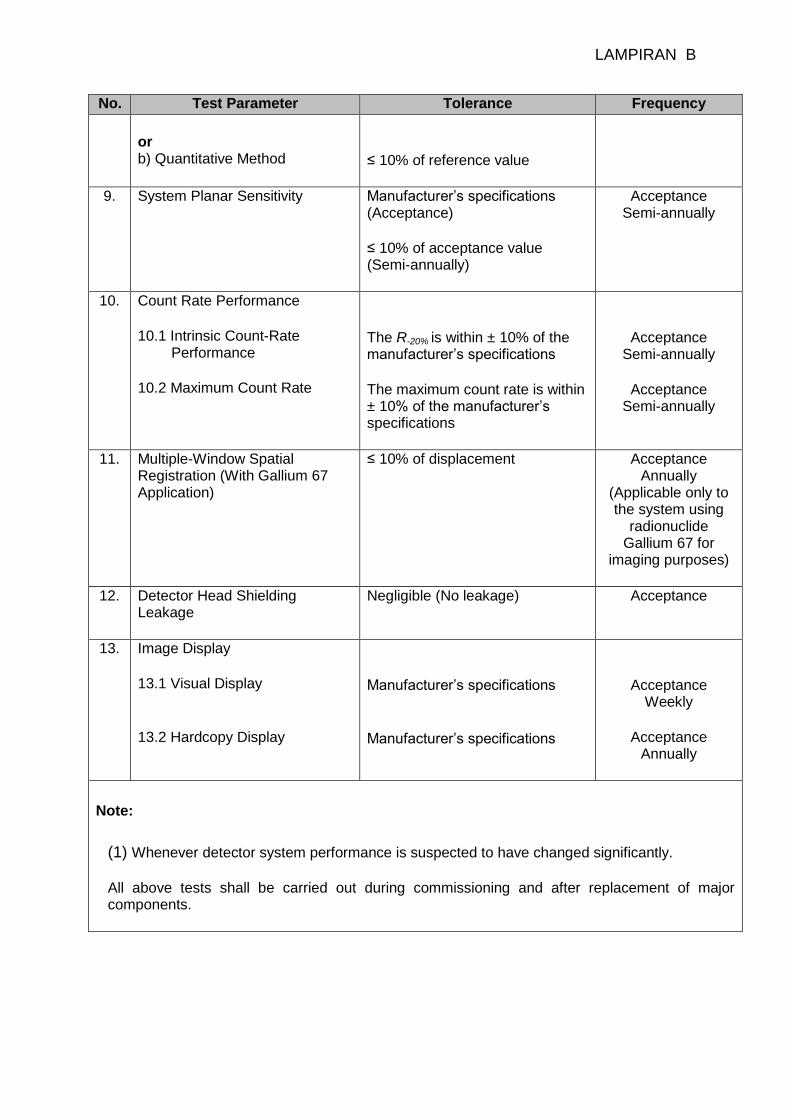
No. Test Parameter Tolerance Frequency
or b) Quantitative Method
≤ 10% of reference value
9.
System Planar Sensitivity Manufacturer’s specifications (Acceptance) ≤ 10% of acceptance value (Semi-annually)
Acceptance Semi-annually
10. Count Rate Performance 10.1 Intrinsic Count-Rate
Performance 10.2 Maximum Count Rate
The R-20% is within ± 10% of the manufacturer’s specifications The maximum count rate is within ± 10% of the manufacturer’s specifications
Acceptance Semi-annually
Acceptance
Semi-annually
11. Multiple-Window Spatial Registration (With Gallium 67 Application)
≤ 10% of displacement Acceptance Annually
(Applicable only to the system using
radionuclide Gallium 67 for
imaging purposes)
12. Detector Head Shielding Leakage
Negligible (No leakage) Acceptance
13. Image Display 13.1 Visual Display 13.2 Hardcopy Display
Manufacturer’s specifications Manufacturer’s specifications
Acceptance Weekly
Acceptance
Annually
Note:
(1) Whenever detector system performance is suspected to have changed significantly. All above tests shall be carried out during commissioning and after replacement of major components.
LAMPIRAN B
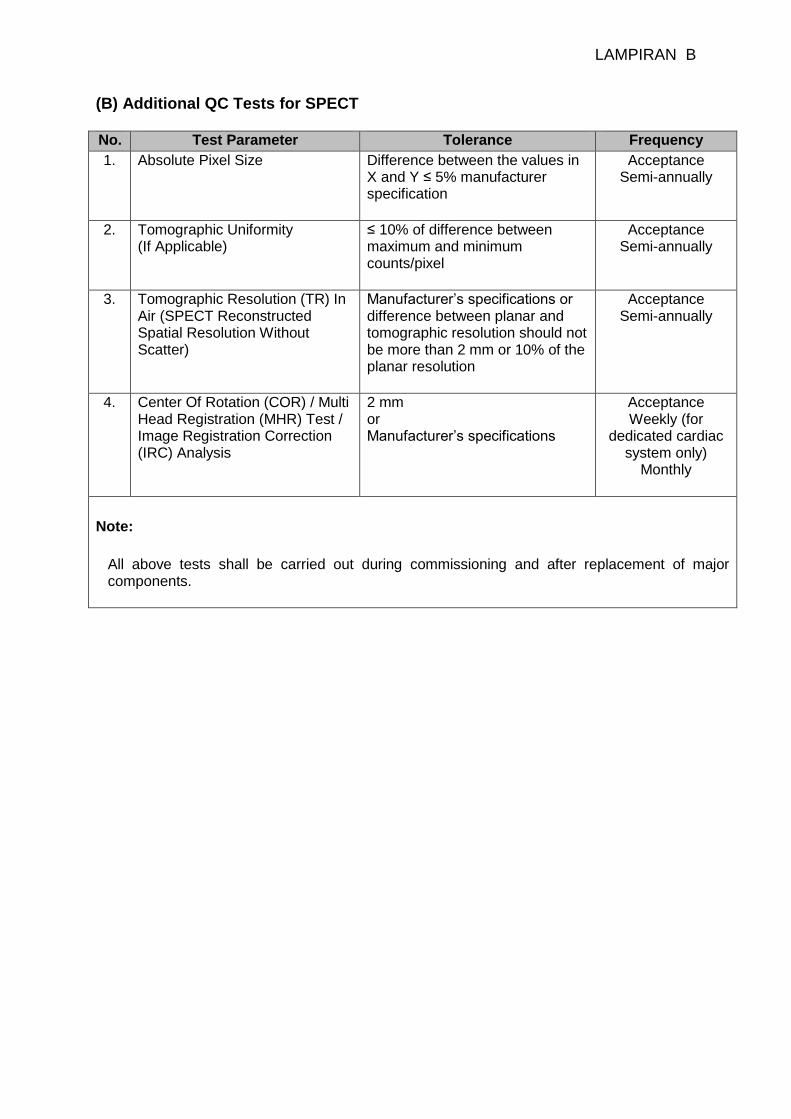
(B) Additional QC Tests for SPECT No. Test Parameter Tolerance Frequency
1. Absolute Pixel Size
Difference between the values in X and Y ≤ 5% manufacturer specification
Acceptance Semi-annually
2. Tomographic Uniformity (If Applicable)
≤ 10% of difference between maximum and minimum counts/pixel
Acceptance Semi-annually
3. Tomographic Resolution (TR) In Air (SPECT Reconstructed Spatial Resolution Without Scatter)
Manufacturer’s specifications or difference between planar and tomographic resolution should not be more than 2 mm or 10% of the planar resolution
Acceptance Semi-annually
4. Center Of Rotation (COR) / Multi Head Registration (MHR) Test / Image Registration Correction (IRC) Analysis
2 mm or Manufacturer’s specifications
Acceptance Weekly (for
dedicated cardiac system only)
Monthly
Note:
All above tests shall be carried out during commissioning and after replacement of major components.
LAMPIRAN B
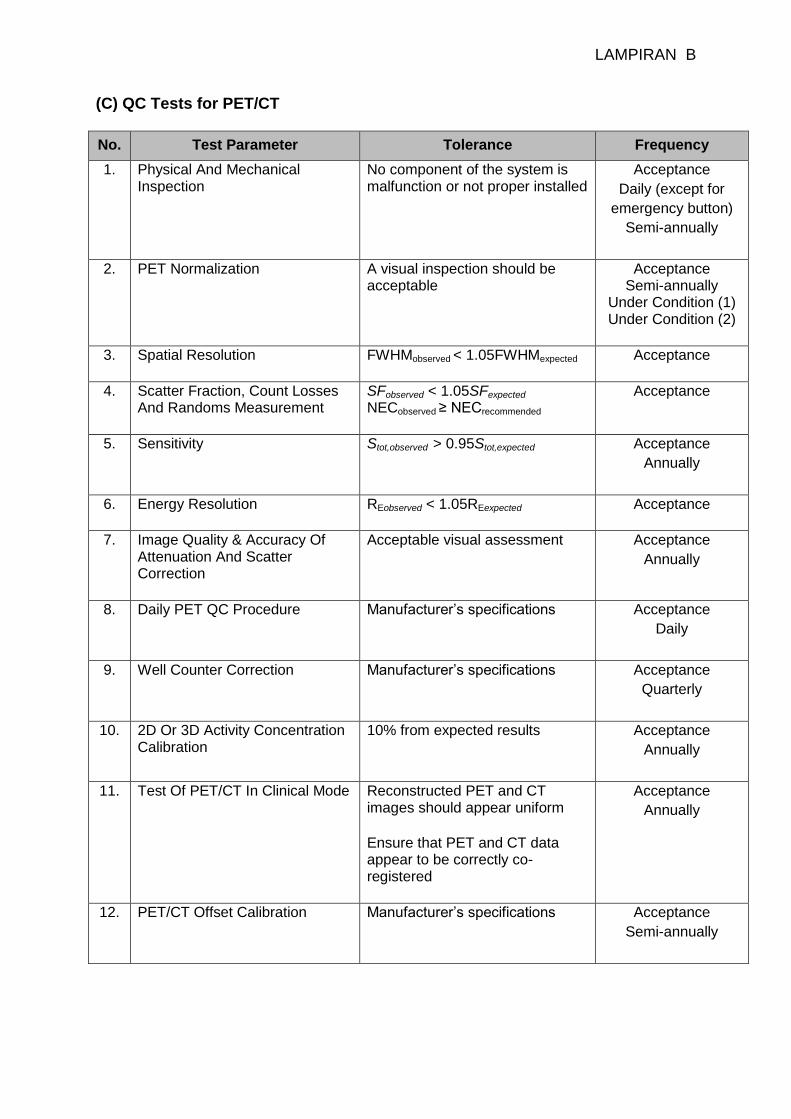
(C) QC Tests for PET/CT
No. Test Parameter Tolerance Frequency
1. Physical And Mechanical Inspection
No component of the system is malfunction or not proper installed
Acceptance
Daily (except for
emergency button)
Semi-annually
2. PET Normalization A visual inspection should be acceptable
Acceptance Semi-annually
Under Condition (1) Under Condition (2)
3. Spatial Resolution FWHMobserved < 1.05FWHMexpected
Acceptance
4. Scatter Fraction, Count Losses And Randoms Measurement
SFobserved < 1.05SFexpected NECobserved ≥ NECrecommended
Acceptance
5. Sensitivity
Stot,observed > 0.95Stot,expected Acceptance
Annually
6. Energy Resolution REobserved < 1.05REexpected
Acceptance
7. Image Quality & Accuracy Of Attenuation And Scatter Correction
Acceptable visual assessment Acceptance
Annually
8. Daily PET QC Procedure Manufacturer’s specifications
Acceptance
Daily
9. Well Counter Correction Manufacturer’s specifications
Acceptance
Quarterly
10. 2D Or 3D Activity Concentration Calibration
10% from expected results Acceptance
Annually
11. Test Of PET/CT In Clinical Mode Reconstructed PET and CT images should appear uniform Ensure that PET and CT data appear to be correctly co-registered
Acceptance
Annually
12. PET/CT Offset Calibration Manufacturer’s specifications
Acceptance
Semi-annually
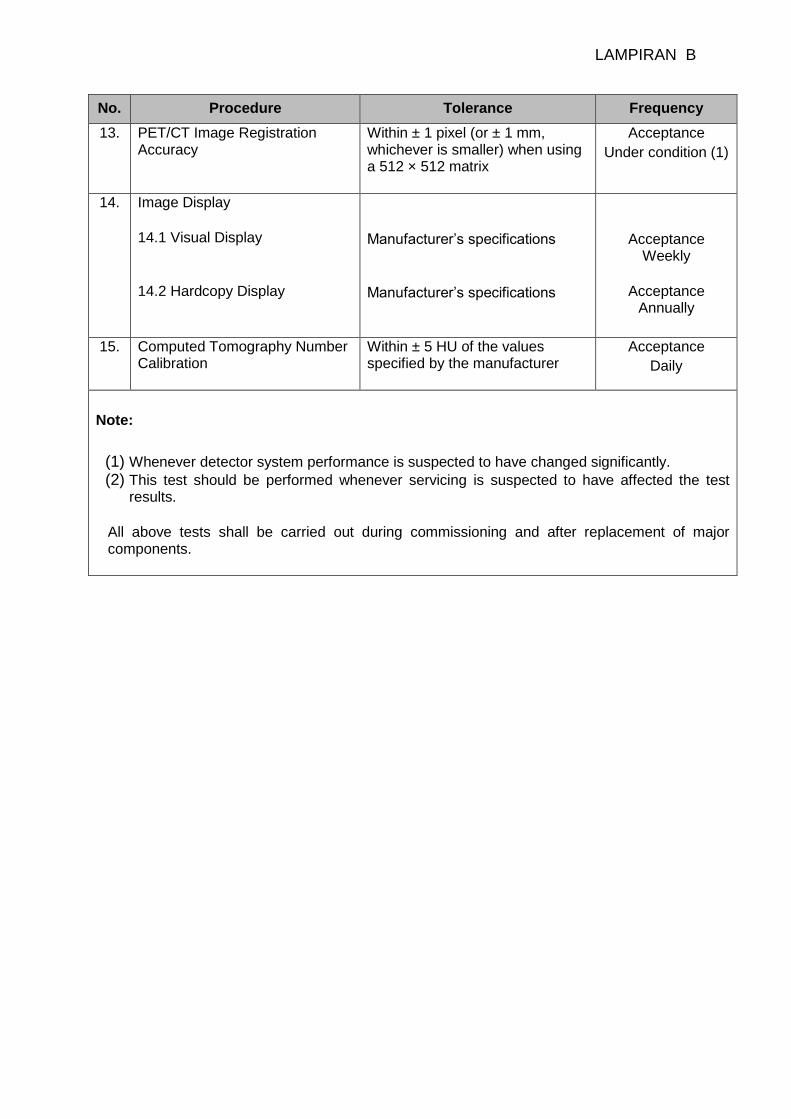
LAMPIRAN B
No. Procedure Tolerance Frequency
13. PET/CT Image Registration Accuracy
Within ± 1 pixel (or ± 1 mm, whichever is smaller) when using a 512 × 512 matrix
Acceptance
Under condition (1)
14. Image Display 14.1 Visual Display 14.2 Hardcopy Display
Manufacturer’s specifications
Manufacturer’s specifications
Acceptance Weekly
Acceptance
Annually
15. Computed Tomography Number Calibration
Within ± 5 HU of the values specified by the manufacturer
Acceptance
Daily
Note:
(1) Whenever detector system performance is suspected to have changed significantly. (2) This test should be performed whenever servicing is suspected to have affected the test
results. All above tests shall be carried out during commissioning and after replacement of major components.
LAMPIRAN B
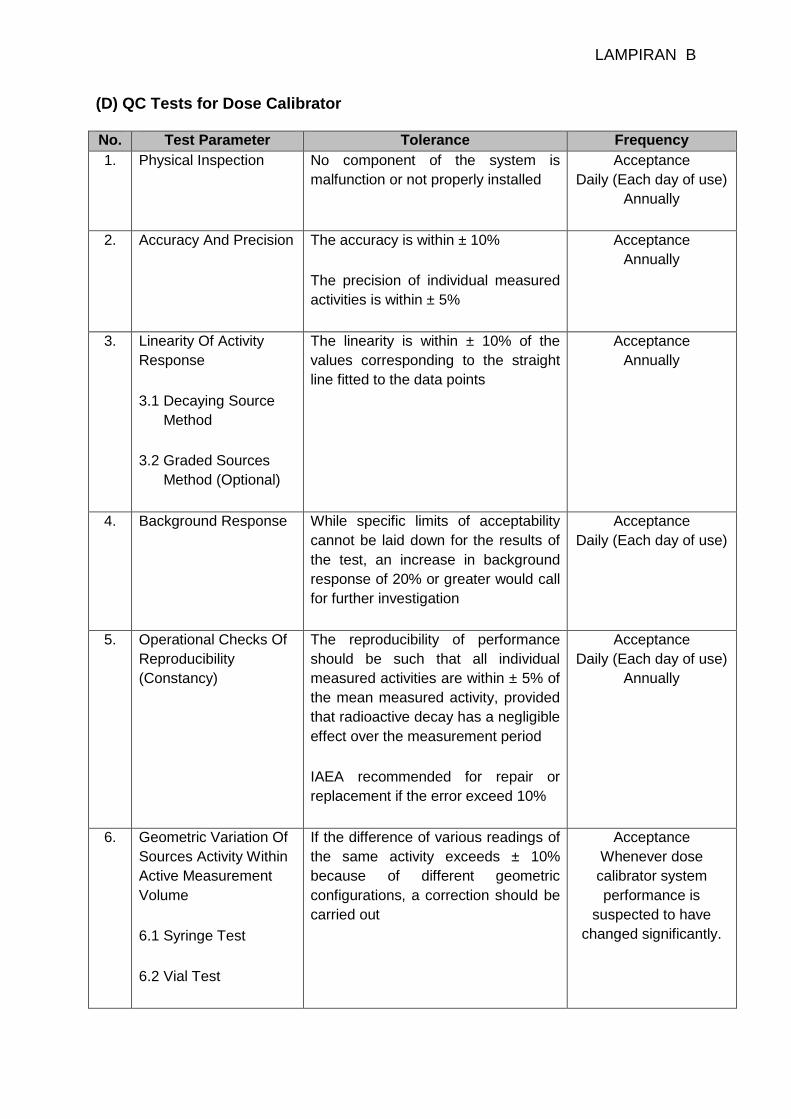
(D) QC Tests for Dose Calibrator No. Test Parameter Tolerance Frequency
1. Physical Inspection No component of the system is
malfunction or not properly installed
Acceptance
Daily (Each day of use)
Annually
2. Accuracy And Precision The accuracy is within ± 10%
The precision of individual measured
activities is within ± 5%
Acceptance
Annually
3. Linearity Of Activity
Response
3.1 Decaying Source
Method
3.2 Graded Sources
Method (Optional)
The linearity is within ± 10% of the
values corresponding to the straight
line fitted to the data points
Acceptance
Annually
4. Background Response While specific limits of acceptability
cannot be laid down for the results of
the test, an increase in background
response of 20% or greater would call
for further investigation
Acceptance
Daily (Each day of use)
5. Operational Checks Of
Reproducibility
(Constancy)
The reproducibility of performance
should be such that all individual
measured activities are within ± 5% of
the mean measured activity, provided
that radioactive decay has a negligible
effect over the measurement period
IAEA recommended for repair or
replacement if the error exceed 10%
Acceptance
Daily (Each day of use)
Annually
6. Geometric Variation Of
Sources Activity Within
Active Measurement
Volume
6.1 Syringe Test
6.2 Vial Test
If the difference of various readings of
the same activity exceeds ± 10%
because of different geometric
configurations, a correction should be
carried out
Acceptance
Whenever dose
calibrator system
performance is
suspected to have
changed significantly.
LAMPIRAN B
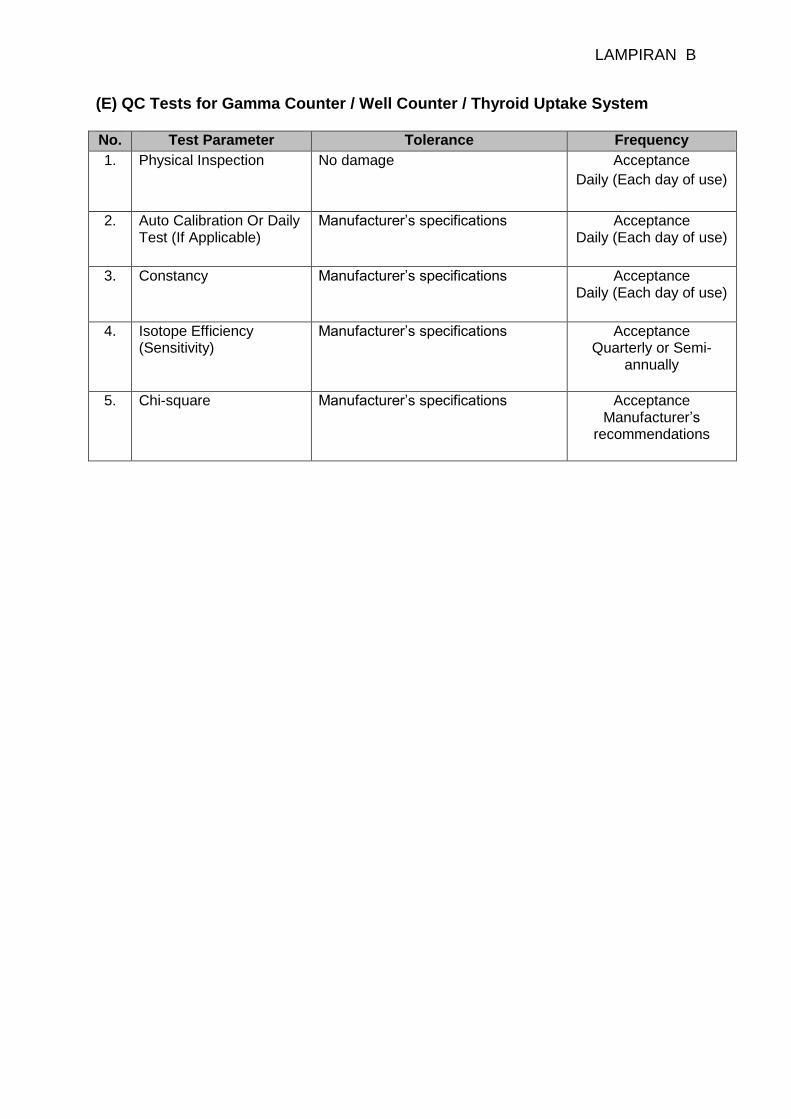
(E) QC Tests for Gamma Counter / Well Counter / Thyroid Uptake System No. Test Parameter Tolerance Frequency
1. Physical Inspection No damage Acceptance
Daily (Each day of use)
2. Auto Calibration Or Daily Test (If Applicable)
Manufacturer’s specifications Acceptance Daily (Each day of use)
3. Constancy Manufacturer’s specifications Acceptance
Daily (Each day of use)
4. Isotope Efficiency
(Sensitivity) Manufacturer’s specifications Acceptance
Quarterly or Semi-annually
5. Chi-square Manufacturer’s specifications Acceptance
Manufacturer’s recommendations
LAMPIRAN B
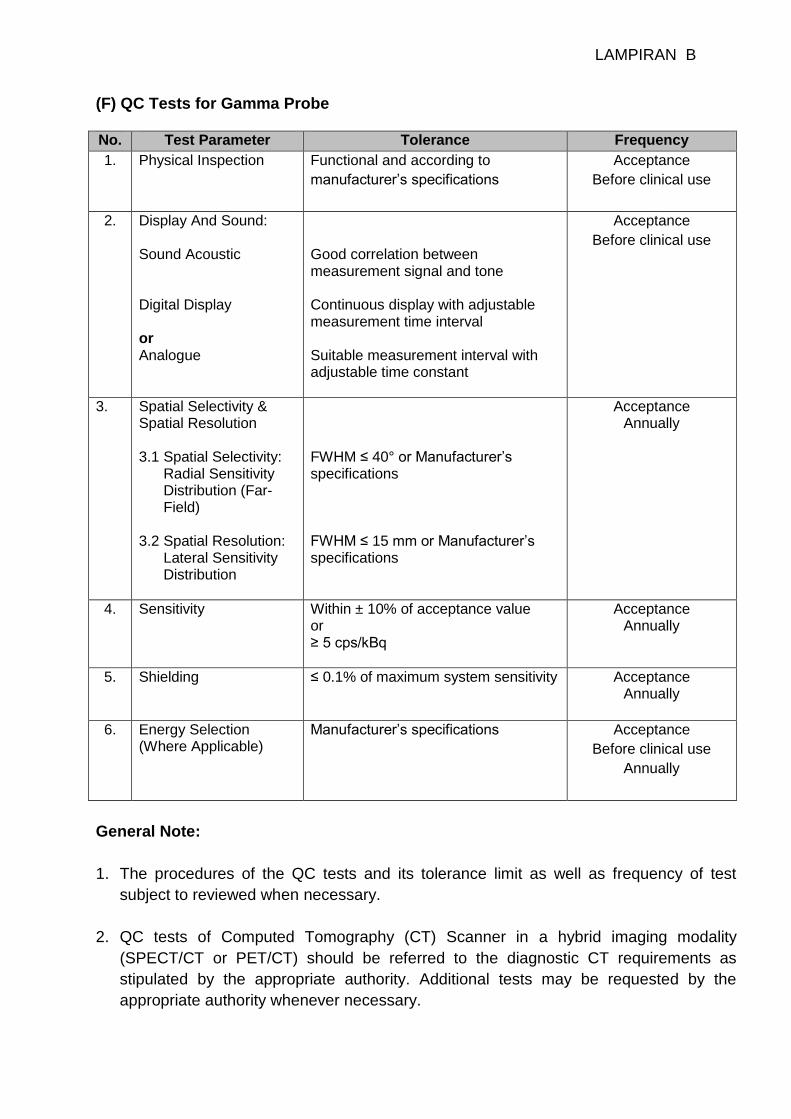
(F) QC Tests for Gamma Probe No. Test Parameter Tolerance Frequency
1. Physical Inspection Functional and according to
manufacturer’s specifications
Acceptance
Before clinical use
2. Display And Sound: Sound Acoustic Digital Display or Analogue
Good correlation between measurement signal and tone Continuous display with adjustable measurement time interval Suitable measurement interval with adjustable time constant
Acceptance
Before clinical use
3. Spatial Selectivity & Spatial Resolution 3.1 Spatial Selectivity: Radial Sensitivity Distribution (Far- Field) 3.2 Spatial Resolution: Lateral Sensitivity Distribution
FWHM ≤ 40° or Manufacturer’s specifications FWHM ≤ 15 mm or Manufacturer’s specifications
Acceptance Annually
4. Sensitivity Within ± 10% of acceptance value or ≥ 5 cps/kBq
Acceptance Annually
5. Shielding ≤ 0.1% of maximum system sensitivity
Acceptance Annually
6. Energy Selection
(Where Applicable) Manufacturer’s specifications Acceptance
Before clinical use
Annually
General Note:
1. The procedures of the QC tests and its tolerance limit as well as frequency of test
subject to reviewed when necessary.
2. QC tests of Computed Tomography (CT) Scanner in a hybrid imaging modality
(SPECT/CT or PET/CT) should be referred to the diagnostic CT requirements as
stipulated by the appropriate authority. Additional tests may be requested by the
appropriate authority whenever necessary.