oktober 2018 management of hyperthyroid page patient...
TRANSCRIPT
BULE
TIN
PENAWAR
VOLUME 3/2018
Oktober 2018
EDITORIAL BOARD ADVISOR: PN HJH ROHAYAH BINTI ABD. GHANI EDITORS: PN SITI ROSNAH BT. SURADI EN MOHD SHAFIE BIN ZABIDI CIK ZANARIAH BT. ABU BAKAR PN NABILAH BT. KAMARUDDIN
HOSPITAL SULTANAH AMINAH JOHOR BAHRU KEMENTERIAN KESIHATAN MALAYSIA JALAN PERSIARAN ABU BAKAR SULTAN 80100 JOHOR BAHRU TEL: 07-2257000 FAX: 07-2242694 EMAIL: [email protected]
IN THIS ISSUE Management of Hyperthyroid
Management of Anaemia in Renal Patient
Attention Deficit Hyperactivity Disorder
PAGE 2-3
PAGE 4-5
PAGE 6-7
PAGE 8-9
Osteoporosis in Postmenopausal Woman
Laporan Majlis Sambutan Hari Raya
Jabatan Farmasi dan Hari Lahir April-Jun
2018
PAGE 10
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 2
By : Nur Hafizah Asikin Binti Mohamed THYROID HORMONE
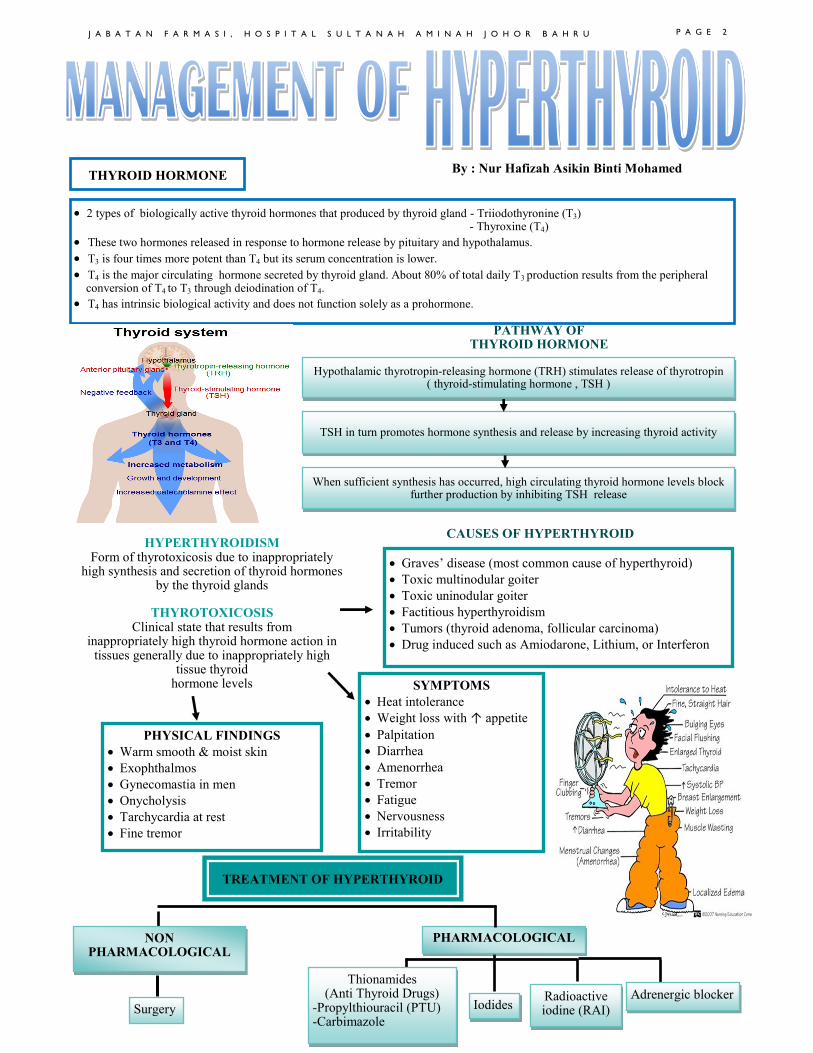
• 2 types of biologically active thyroid hormones that produced by thyroid gland - Triiodothyronine (T3) - Thyroxine (T4)
• These two hormones released in response to hormone release by pituitary and hypothalamus.
• T3 is four times more potent than T4 but its serum concentration is lower.
• T4 is the major circulating hormone secreted by thyroid gland. About 80% of total daily T3 production results from the peripheral conversion of T4 to T3 through deiodination of T4.
• T4 has intrinsic biological activity and does not function solely as a prohormone.
PATHWAY OF THYROID HORMONE
Hypothalamic thyrotropin-releasing hormone (TRH) stimulates release of thyrotropin ( thyroid-stimulating hormone , TSH )
TSH in turn promotes hormone synthesis and release by increasing thyroid activity
When sufficient synthesis has occurred, high circulating thyroid hormone levels block further production by inhibiting TSH release
HYPERTHYROIDISM Form of thyrotoxicosis due to inappropriately
high synthesis and secretion of thyroid hormones by the thyroid glands
THYROTOXICOSIS
Clinical state that results from inappropriately high thyroid hormone action in
tissues generally due to inappropriately high tissue thyroid
hormone levels
• Graves’ disease (most common cause of hyperthyroid)
• Toxic multinodular goiter
• Toxic uninodular goiter
• Factitious hyperthyroidism
• Tumors (thyroid adenoma, follicular carcinoma)
• Drug induced such as Amiodarone, Lithium, or Interferon
CAUSES OF HYPERTHYROID
SYMPTOMS
• Heat intolerance
• Weight loss with ↑ appetite
• Palpitation
• Diarrhea
• Amenorrhea
• Tremor
• Fatigue
• Nervousness
• Irritability
PHYSICAL FINDINGS
• Warm smooth & moist skin
• Exophthalmos
• Gynecomastia in men
• Onycholysis
• Tarchycardia at rest
• Fine tremor
Thionamides (Anti Thyroid Drugs)
-Propylthiouracil (PTU) -Carbimazole
TREATMENT OF HYPERTHYROID
NON PHARMACOLOGICAL
Surgery
PHARMACOLOGICAL
Radioactive iodine (RAI) Iodides
Adrenergic blocker
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 3
CONSIDER IN PATIENT– -Large thyroid gland (>80g) -Lack of remission on antithyroid drug treatment -Severe ophthalmopathy -Pregnant and children who have had major adverse reactions to antithyroid drugs -Can be used for patients who are noncompliant and refuse radioactive iodine
SURGERY
RADIOACTIVE IODINE (RAI)
•Sodium iodide – 131 → oral liquid / capsule that concentrates in the thyroid and initially disrupts hormone synthesis •Contraindicated in pregnancy
IODIDES
MODE OF ACTION -Acutely blocks thyroid hormone release -↓ size and vascularity of the glands -Inhibits thyroid hormone biosynthesis DOSE AND MONITORING Potassium iodide →available as a saturated solution OR → 38mg iodide per drop
Lugol’s solution → containing 6.3mg of iodide per drop → 1ml contain 50mg free iodine & about 130mg total iodine •Daily dose – 1ml daily in divided doses / 5 – 10 drops TDS •It should be administered 7 to 14 days preoperatively & not to be used for long term treatment
ANTI THYROID DRUGS
MOST USEFUL IN
PROPYLTHIOURACIL CARBIMAZOLE
Initial dose 300-450mg in 8 hourly interval 10 – 60mg daily in divided doses given 8 hourly
Maintenance dose 50-150mg in every 8 hours for at least 12-18 months
5 – 20mg daily for at least 12 – 18 months
Maximum dose 1200mg/day 60mg daily
Dose for pediatrics 50/m2 8 hourly Maintenance : 1/3 to 2/3 of the initial dose
0.4mg/kg/day 8-12 hourly oral for 2 weeks then 0.1mg/kg 8-24 hourly
Special population Preferred in pregnancy Max 450mg/day in 3 divided doses
Pregnancy-intolerance to PTU Max 20-30mg given daily
Precaution Not considered as first line therapy → serious hepatotoxicity
-
ADRENERGIC BLOCKER
-Used to ameliorate thyrotoxic symptoms such as palpitations, anxiety, tremor and heat intolerance DOSE AND MONITORING
• Propranolol 10-40mg TDS/QID → may block T4 to T3 conversion at high doses
• Alternatives to control symptoms when β-blocker is contraindicated → calcium channel antagonist - PO Diltiazem 120mg TDS - PO Verapamil 80-120mg TDS/QID
References: 1. Koda-Kimble MA et al., Applied Therapeutics. The Clinical Use of Drugs. 9th Edition. Wolters Kluwer Health 2. DiPiro JT et al., Pharmacotherapy Handbook. A Pathophysiologic Approach. 9th Edition. Mc Graw HillSoo HH et al., (2017). 3. Sarawak Handbook of Medical Emergencies. 3rd Edition. CE Publishing 4. Alexander EK et al., Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. American Thyroid Association, 27th edition (3). 6. Bahn RS et al., (2011). Hyperthyroidism And Other Causes Of Thyrotoxicosis. Management Guidelines Of The American Thyroid Association And American Association Of Clinical Endocrinologist, 23th edition (3). 7. Abdul Ghandour et al., (2011). Hyperthyroidism : A Stepwise Approach to Management. The Journal of Family Practice, 60th edition (7).
PREFERRED TREATMENT DOSE & MONITORING
-Elderly or patient with cardiac comorbidities who are poor surgical candidates -Fail to respond to drug therapy / experienced adverse drug therapy -Developed recurrent hyperthyroidism after surgery
-Usually given in a single dose – maximal benefit is noted within 3 to 6 months -Single dose of 5 – 30 milicuries -Second dose of RAI given 6 months after the first RAI treatment – if patient remain hyperthyroid
•This surgery preserves some of the thyroid tissue and reduces the incidence of hypothyroidism to 25%. However, persistent or recurrent hyperthyroidism occurs in 8% of patients •Total thyroidectomy is reserved for patients with severe disease or large goiters in whom recurrences would be highly problematic
INDICATION -Preoperative preparation before surgery -Provides symptomatic relief of hyperthyroid symptoms -Thyroid storm -Contraindicated in pregnancy
-Children & pregnant women -Patients with contraindication to surgery or refused surgery
-Patients who relapse after thyroidectomy -Patients in preparation for surgery or awaiting radioiodine therapy
-Patients with medical complication
MANAGEMENT OF ANAEMIA IN RENAL PATIENT B Y : W O N G J I N N I
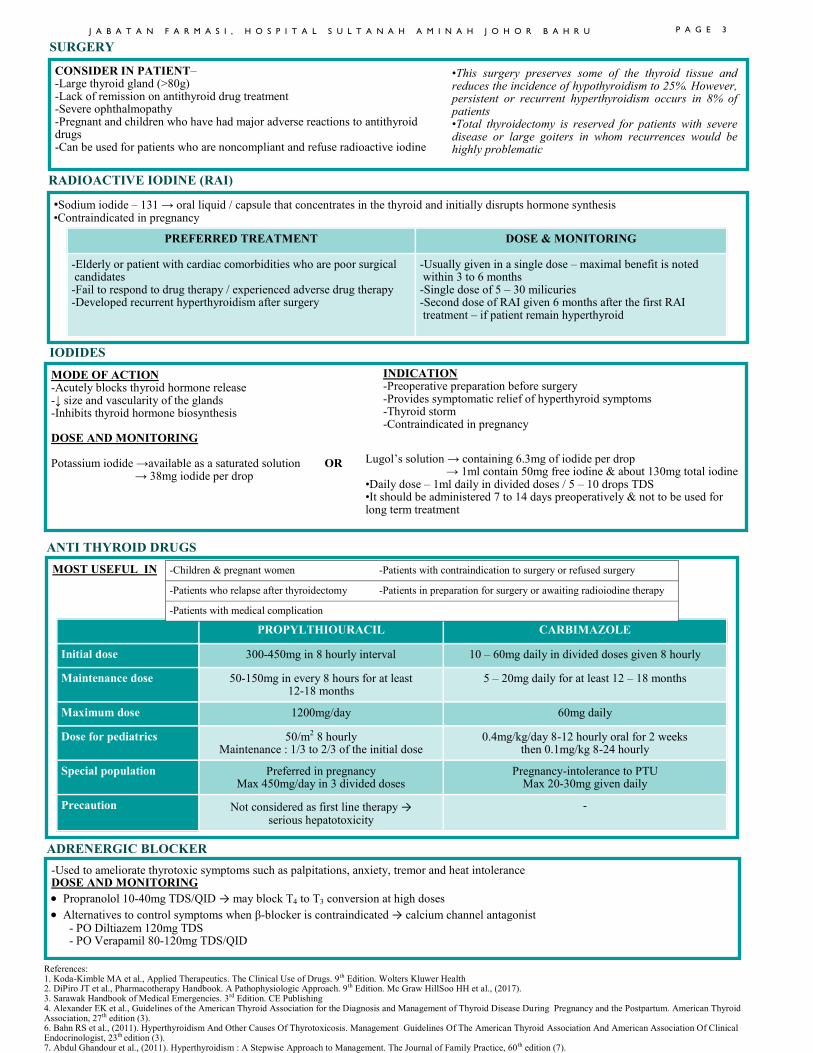
DEFINITION OF CHRONIC KIDNEY DISEASE (CKD)
• Kidney damage for ≥3 months, as de-fined by structural or functional abnor-malities of the kidney, with or without decreased Glomerular Filtration Rate (GFR), manifest by either:
Pathological abnormalities; or
Markers of kidney damage, in-cluding abnormalities in the com-position of blood or urine, or abnormalities in imaging tests
• GFR <60min/ml/1.73m2 ≥ 3 months, with or without kidney damage
DEFINITION OF ANAEMIA
• <13.0 g/dL for adult males
• <12.0 g/dL for adult females
Normally present as normochromic normocytic anaemia
IRON THERAPY
• To treat iron deficiency
• Increase Hb level with/without ESA
• Prevent anaemia development in ESA treated patients
• Reduce ESA doses in ESA-treated patients
CAUSES OF ANAEMIA
• Less erythropoietin production
• Shorter life span of RBCs
• Dialysis induced blood & iron loss
• Vitamin B12 deficiency
• Systemic infection / inflammatory dis-eases
• Severe hyperparathyroidism
• Aluminium overload
• Haemoglobinopathies
• Hypothyroidism
• Drug induced hemolytic anaemia
TREATMENT GOALS
• Reduce left ventricular hypertrophy
• Decrease morbidity/mortality
• Increase exercise tolerance
• Increase quality of life
Parameters Evaluation
Haemoglobin Degree of anaemia
Mean Corpuscular Volume (MCV) Mean Corpuscular Hemoglobin Concen-tration (MCHC)
Type of anemia
Serum ferritin Iron stores
Serum iron Total Iron Binding Capacity (TIBC) %Transferrin Satura-tion (TSAT)
Functional iron avail-able for erythropoie-sis.
Vitamin B12 and Folate
Type of anaemia
Plasma or serum C-reactive protein (CRP)
Inflammation
Stool occult blood Presence of ongoing GI bleeding or ulcer-ation
TREATMENT OPTIONS
1) Iron
2) Erythropoietin stimulating agent (ESA)
3) Blood transfusion
General approach:
• Functional iron deficiency (ferritin>100ng/mL): Start with Iron; then +ESA (if Hb<11) OR reduce Iron (if Hb>11)
• Absolute iron deficiency (ferritin<100ng/mL): Iron + ESA
IV Iron Oral Iron
• Recommended for all CKD patients especially haemodialy-sis patients due to chronic blood loss
• Adverse effects: Anaphylactic reaction
• Recommended in non-dialysis or peritoneal dialysis patient due to less blood loss and without IV access
• Limited by poor absorption and non-adherence due to adverse effects
• Example: Ferrous fumarate 200mg tablet
• Adverse effects: dizziness, chest pain, palpitation, flushing, abdominal pain
•Recommended oral iron dose: 200mg elemental iron/day Should be taken before food/empty stomach as acidic environment promotes ionization of iron making it easier to be absorbed
Monitoring Parameters
Minimum target
Optimal target Maximum target
Serum ferritin ≥100ng/mL 200-500ng/mL >800ng/mL
TSAT >20% 30-40% >50%
% hypochromic red cells <10% <2.5%
ANAEMIA WORK-UP
MONITORING IRON STATUS Evaluate TSAT and ferritin ≤ every 3 months during ESA therapy, including the decision to start or continue therapy. Evaluation must be more frequent when:
• Initiating or increasing ESA dose
• There is blood loss
• In other circumstances where iron stores may become depleted
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 4
B Y : W O N G
J I N N I
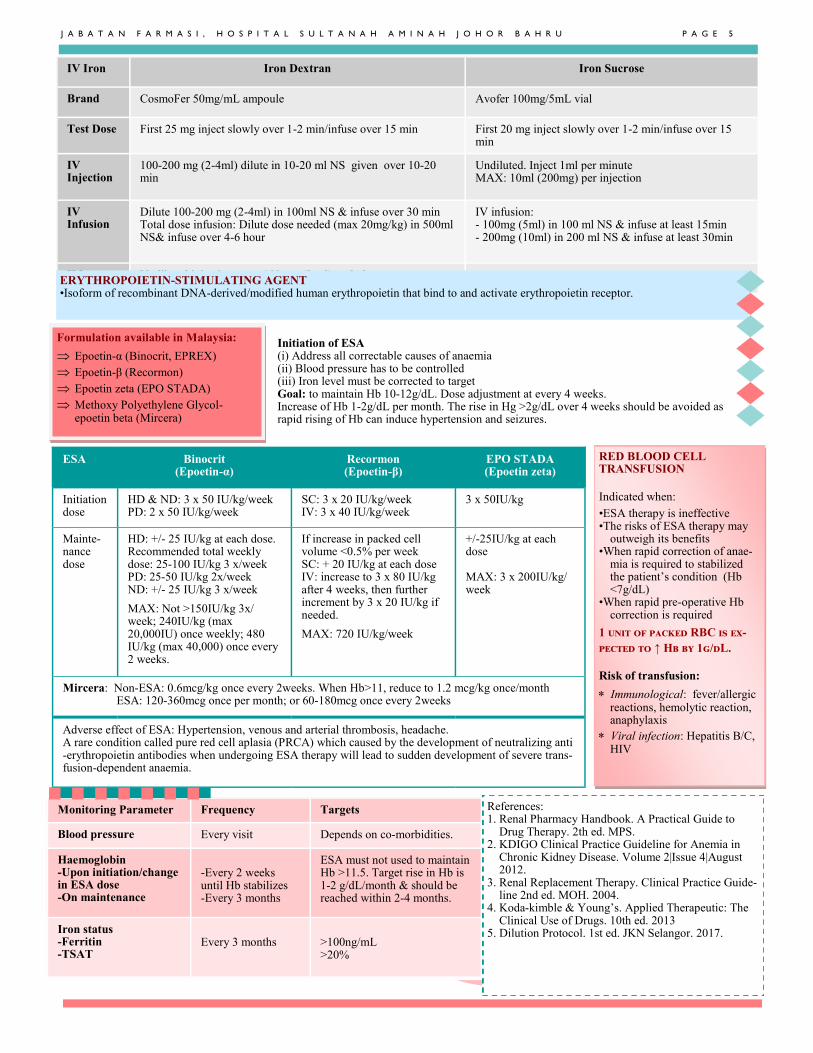
IV Iron Iron Dextran Iron Sucrose
Brand CosmoFer 50mg/mL ampoule Avofer 100mg/5mL vial
Test Dose First 25 mg inject slowly over 1-2 min/infuse over 15 min First 20 mg inject slowly over 1-2 min/infuse over 15 min
IV Injection
100-200 mg (2-4ml) dilute in 10-20 ml NS given over 10-20 min
Undiluted. Inject 1ml per minute MAX: 10ml (200mg) per injection
IV Infusion
Dilute 100-200 mg (2-4ml) in 100ml NS & infuse over 30 min Total dose infusion: Dilute dose needed (max 20mg/kg) in 500ml NS& infuse over 4-6 hour
IV infusion: - 100mg (5ml) in 100 ml NS & infuse at least 15min - 200mg (10ml) in 200 ml NS & infuse at least 30min
IM Undiluted injection up to 100 mg (2 ml) each dose - ERYTHROPOIETIN-STIMULATING AGENT •Isoform of recombinant DNA-derived/modified human erythropoietin that bind to and activate erythropoietin receptor.
ESA Binocrit (Epoetin-α)
Recormon (Epoetin-β)
EPO STADA (Epoetin zeta)
Initiation dose
HD & ND: 3 x 50 IU/kg/week PD: 2 x 50 IU/kg/week
SC: 3 x 20 IU/kg/week IV: 3 x 40 IU/kg/week
3 x 50IU/kg
Mainte-nance dose
HD: +/- 25 IU/kg at each dose. Recommended total weekly dose: 25-100 IU/kg 3 x/week PD: 25-50 IU/kg 2x/week ND: +/- 25 IU/kg 3 x/week MAX: Not >150IU/kg 3x/week; 240IU/kg (max 20,000IU) once weekly; 480 IU/kg (max 40,000) once every 2 weeks.
If increase in packed cell volume <0.5% per week SC: + 20 IU/kg at each dose IV: increase to 3 x 80 IU/kg after 4 weeks, then further increment by 3 x 20 IU/kg if needed. MAX: 720 IU/kg/week
+/-25IU/kg at each dose MAX: 3 x 200IU/kg/week
Mircera: Non-ESA: 0.6mcg/kg once every 2weeks. When Hb>11, reduce to 1.2 mcg/kg once/month ESA: 120-360mcg once per month; or 60-180mcg once every 2weeks
Adverse effect of ESA: Hypertension, venous and arterial thrombosis, headache. A rare condition called pure red cell aplasia (PRCA) which caused by the development of neutralizing anti-erythropoietin antibodies when undergoing ESA therapy will lead to sudden development of severe trans-fusion-dependent anaemia.
Monitoring Parameter Frequency Targets
Blood pressure Every visit Depends on co-morbidities.
Haemoglobin -Upon initiation/change in ESA dose -On maintenance
-Every 2 weeks until Hb stabilizes -Every 3 months
ESA must not used to maintain Hb >11.5. Target rise in Hb is 1-2 g/dL/month & should be reached within 2-4 months.
Iron status -Ferritin -TSAT
Every 3 months
>100ng/mL >20%
RED BLOOD CELL TRANSFUSION
Indicated when:
•ESA therapy is ineffective •The risks of ESA therapy may
outweigh its benefits •When rapid correction of anae-
mia is required to stabilized the patient’s condition (Hb <7g/dL)
•When rapid pre-operative Hb correction is required
1 unit of packed RBC is ex-
pected to ↑ Hb by 1g/dL.
Risk of transfusion:
Immunological: fever/allergic reactions, hemolytic reaction, anaphylaxis
Viral infection: Hepatitis B/C, HIV
Initiation of ESA (i) Address all correctable causes of anaemia (ii) Blood pressure has to be controlled (iii) Iron level must be corrected to target Goal: to maintain Hb 10-12g/dL. Dose adjustment at every 4 weeks. Increase of Hb 1-2g/dL per month. The rise in Hg >2g/dL over 4 weeks should be avoided as rapid rising of Hb can induce hypertension and seizures.
Formulation available in Malaysia:
Epoetin-α (Binocrit, EPREX)
Epoetin-β (Recormon)
Epoetin zeta (EPO STADA)
Methoxy Polyethylene Glycol-epoetin beta (Mircera)
References: 1. Renal Pharmacy Handbook. A Practical Guide to
Drug Therapy. 2th ed. MPS. 2. KDIGO Clinical Practice Guideline for Anemia in
Chronic Kidney Disease. Volume 2|Issue 4|August 2012.
3. Renal Replacement Therapy. Clinical Practice Guide-line 2nd ed. MOH. 2004.
4. Koda-kimble & Young’s. Applied Therapeutic: The Clinical Use of Drugs. 10th ed. 2013
5. Dilution Protocol. 1st ed. JKN Selangor. 2017.
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 5
OSTEOPOROSIS IN POSTMENOPAUSAL WOMAN
B Y : T A N K E L E E N
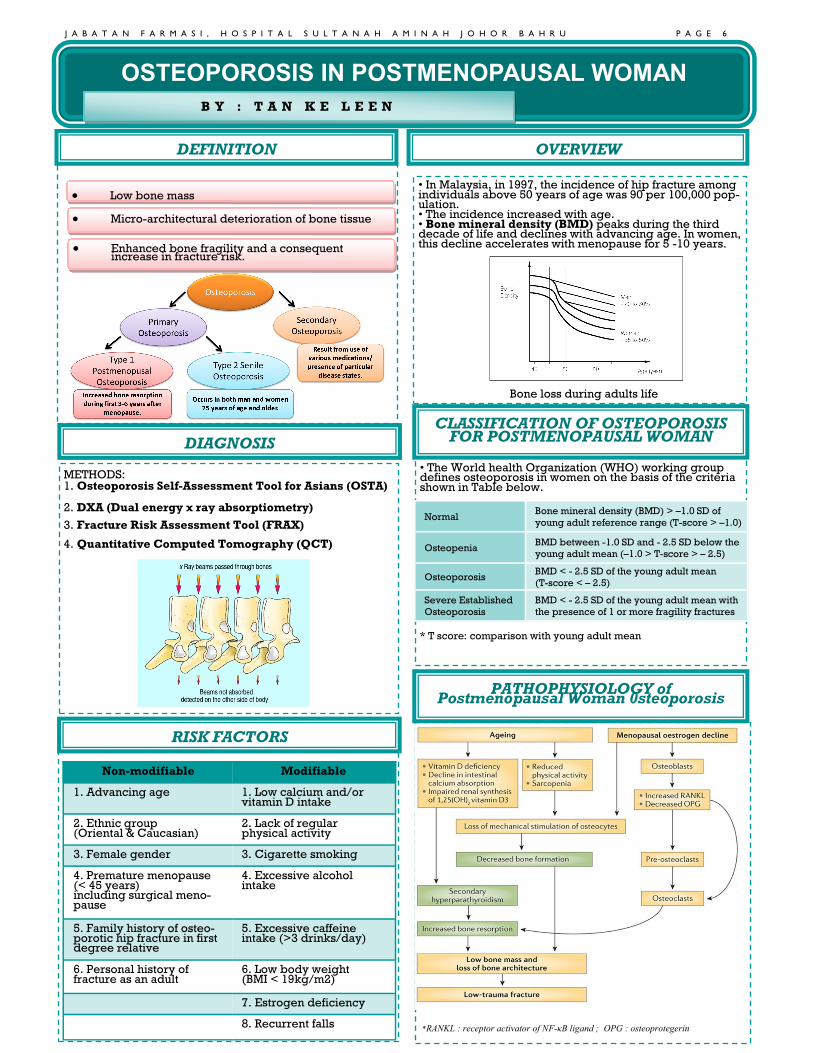
DEFINITION
• Low bone mass
• Micro-architectural deterioration of bone tissue
• Enhanced bone fragility and a consequent increase in fracture risk.
OVERVIEW
• In Malaysia, in 1997, the incidence of hip fracture among individuals above 50 years of age was 90 per 100,000 pop-ulation. • The incidence increased with age. • Bone mineral density (BMD) peaks during the third decade of life and declines with advancing age. In women, this decline accelerates with menopause for 5 -10 years.
METHODS: 1. Osteoporosis Self-Assessment Tool for Asians (OSTA) 2. DXA (Dual energy x ray absorptiometry) 3. Fracture Risk Assessment Tool (FRAX) 4. Quantitative Computed Tomography (QCT)
*RANKL : receptor activator of NF-κB ligand ; OPG : osteoprotegerin
DIAGNOSIS
• The World health Organization (WHO) working group defines osteoporosis in women on the basis of the criteria shown in Table below.
* T score: comparison with young adult mean
Non-modifiable Modifiable
1. Advancing age 1. Low calcium and/or vitamin D intake
2. Ethnic group (Oriental & Caucasian)
2. Lack of regular physical activity
3. Female gender 3. Cigarette smoking
4. Premature menopause (< 45 years) including surgical meno-pause
4. Excessive alcohol intake
5. Family history of osteo-porotic hip fracture in first degree relative
5. Excessive caffeine intake (>3 drinks/day)
6. Personal history of fracture as an adult
6. Low body weight (BMI < 19kg/m2)
7. Estrogen deficiency
8. Recurrent falls
CLASSIFICATION OF OSTEOPOROSIS FOR POSTMENOPAUSAL WOMAN
RISK FACTORS
Bone loss during adults life
PATHOPHYSIOLOGY of Postmenopausal Woman 0steoporosis
Normal Bone mineral density (BMD) > –1.0 SD of
young adult reference range (T-score > –1.0)
Osteopenia BMD between -1.0 SD and - 2.5 SD below the
young adult mean (–1.0 > T-score > – 2.5)
Osteoporosis BMD < - 2.5 SD of the young adult mean
(T-score < – 2.5)
Severe Established
Osteoporosis
BMD < - 2.5 SD of the young adult mean with
the presence of 1 or more fragility fractures
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 6

ALGORITHM FOR MANAGEMENT OF POSTMENOPAUSAL OSTEOPOROSIS
TREATMENT
References: 1.Clinical guidance on management of osteoporosis 2nd edition (2015). 2.Barbara G, Joseph T, Terry L, Cecily V. Pharmacotherapy Handbook. 7º edição. 2009:98-103. 3.Koda-Kimble MA. Koda-Kimble and Young's applied therapeutics: the clinical use of drugs. Lippincott Williams & Wilkins; 2012 Feb 1. 4.Compston J. Guidelines for the management of osteoporosis: the present and the future. Osteoporosis international. 2005 Oct 1;16(10):1173-6. 5.Lexicomp drug reference handbook 24th edition. 6.Lee JK, Khir AS. The incidence of hip fracture in Malaysians above 50 years of age: variation in different ethnic groups. International Journal of Rheumatic Diseas-
Drug Dose
Vitamin D
Alfacalcidol Initial dose: 1mcg daily
Maintenance:0.25-2 mcg daily
Calcitriol 0.25mcg 2 times daily
Hormone therapy
Conjugated estrogen tablet (Premarin) 0.3-0.625mg daily
Conjugated estrogen 0.625mg &
Medroxyprogesteron acetate 2.5mg tablet (Premelle 2.5) 1 tab daily
Estradiol 1mg/Dydrogesterone 5mg tablet (Fermoston 1/5) 1 tab daily
Selective Estrogen Receptor Modulators (SERMs)
Raloxifene 60mg daily
Bisphophonate
Alendronate (Fosamax, Fosamax plus D)
Prevention: 5 mg daily, 35 mg weekly
Treatment: 10 mg daily or 70 mg tablet, 70mg tablet
with vitamin D 2,800 or 5,600 units weekly
Risedronate (Actonel) 5 mg daily; 35 mg weekly; 75 mg on two consecutive
days once monthly; 150 mg monthly
Ibandronate (Boniva) 5mg IV yearly
Zoledronic acid (Reclast) 5mg IV yearly
Calcitonin 200 units intranasal daily, alternating nares every other
day
Bone modifying agent
Denosumab S/C 60mg once every 6months
Recombinant human PTH 1-34 (r-PTH)
Teriparatide S/C 20mcg OD
Strontium Salt
Strontium Ranelate 2g/day dissolved in water, prior to bedtime
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 7

Inattention Hyperactivity
Impulsivity
Trouble sitting still
Runs or climbs at inappropriate times
Trouble playing quietly
Often “on the go,” acts as if “driven by a motor”
Talks excessively
Inattention to detail, makes careless mis-takes.
Trouble staying focused and on task
Not listening
Not following instructions or tasks
Disorganized
Avoids and dislikes task that require sus-tained effort
Loses things
Easily distracted
Forgetful
Blurts out answers before a question has been completed
Difficulty waiting his/her turn
Interrupts or intrudes others
6 (5 in adults) or more symptoms
Predominantly Inattentive Presentation Predominantly Hyperactive/Impulsive Presentation
6 (5 in adults) or more symptoms
Combined Presentation
- Abnormalities in
frontostriatal circuitry.
Brain Function & Structures
- Low level of dopamine and
noradrenaline.
Neurotransmitters Level
- 30-35% of first degree relatives
of children with ADHD.
Gene and Heredity
- Premature birth, maternal
smoking, lead exposure/toxicity.
Environmental Factors
By: Annie Lee Pei Wen
Pharmacological Treatment of
Attention Deficit Hyperactivity Disorder
INTRODUCTION
ETIOLOGICAL
FACTORS
DIAGNOSTIC CRITERIA
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 8
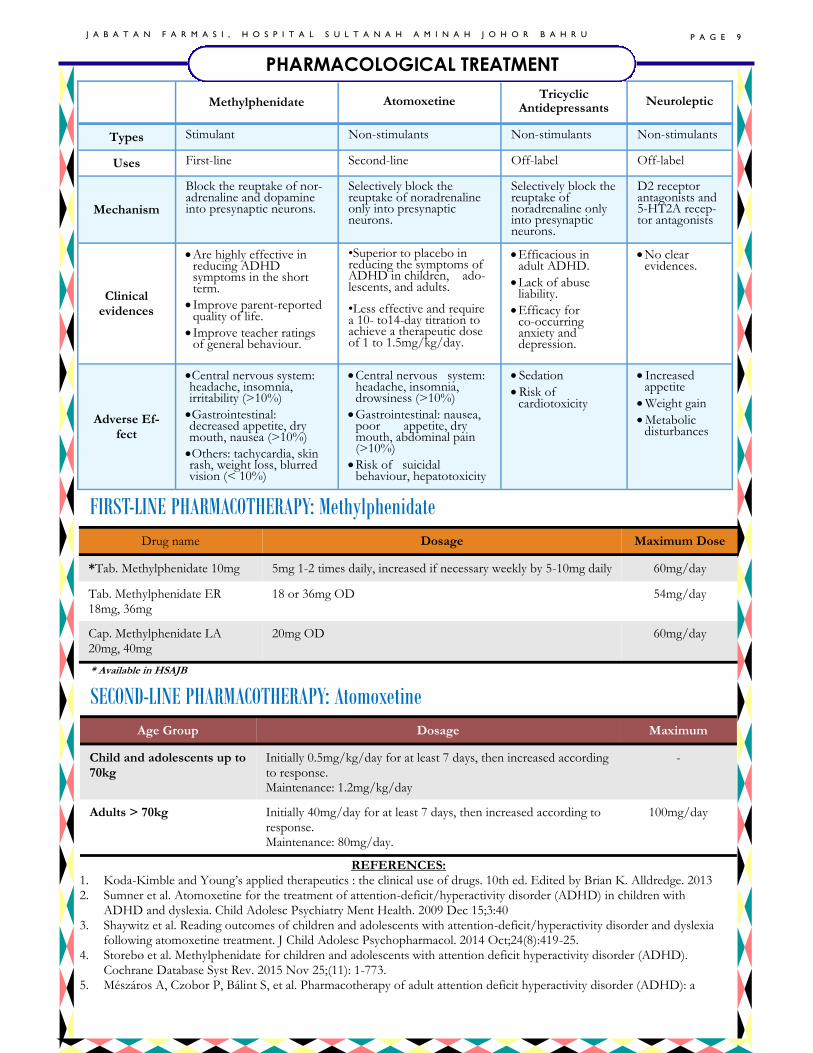
Drug name Dosage Maximum Dose
*Tab. Methylphenidate 10mg 5mg 1-2 times daily, increased if necessary weekly by 5-10mg daily 60mg/day
Tab. Methylphenidate ER 18mg, 36mg
18 or 36mg OD 54mg/day
Cap. Methylphenidate LA 20mg, 40mg
20mg OD 60mg/day
FIRST-LINE PHARMACOTHERAPY: Methylphenidate
* Available in HSAJB
Age Group Dosage Maximum
Child and adolescents up to 70kg
Initially 0.5mg/kg/day for at least 7 days, then increased according to response. Maintenance: 1.2mg/kg/day
-
Adults > 70kg Initially 40mg/day for at least 7 days, then increased according to response. Maintenance: 80mg/day.
100mg/day
SECOND-LINE PHARMACOTHERAPY: Atomoxetine
REFERENCES: 1. Koda-Kimble and Young’s applied therapeutics : the clinical use of drugs. 10th ed. Edited by Brian K. Alldredge. 2013 2. Sumner et al. Atomoxetine for the treatment of attention-deficit/hyperactivity disorder (ADHD) in children with
ADHD and dyslexia. Child Adolesc Psychiatry Ment Health. 2009 Dec 15;3:40 3. Shaywitz et al. Reading outcomes of children and adolescents with attention-deficit/hyperactivity disorder and dyslexia
following atomoxetine treatment. J Child Adolesc Psychopharmacol. 2014 Oct;24(8):419-25. 4. Storebø et al. Methylphenidate for children and adolescents with attention deficit hyperactivity disorder (ADHD).
Cochrane Database Syst Rev. 2015 Nov 25;(11): 1-773. 5. Mészáros A, Czobor P, Bálint S, et al. Pharmacotherapy of adult attention deficit hyperactivity disorder (ADHD): a
Methylphenidate Atomoxetine Tricyclic
Antidepressants Neuroleptic
Types Stimulant Non-stimulants Non-stimulants Non-stimulants
Uses First-line Second-line Off-label Off-label
Mechanism
Block the reuptake of nor-adrenaline and dopamine into presynaptic neurons.
Selectively block the reuptake of noradrenaline only into presynaptic neurons.
Selectively block the reuptake of noradrenaline only into presynaptic neurons.
D2 receptor antagonists and 5-HT2A recep-tor antagonists
Clinical evidences
• Are highly effective in reducing ADHD symptoms in the short term.
• Improve parent-reported quality of life.
• Improve teacher ratings of general behaviour.
•Superior to placebo in reducing the symptoms of ADHD in children, ado-lescents, and adults.
•Less effective and require a 10- to14-day titration to achieve a therapeutic dose of 1 to 1.5mg/kg/day.
• Efficacious in adult ADHD.
• Lack of abuse liability.
• Efficacy for co-occurring anxiety and depression.
• No clear evidences.
Adverse Ef-fect
•Central nervous system: headache, insomnia, irritability (>10%)
•Gastrointestinal: decreased appetite, dry mouth, nausea (>10%)
•Others: tachycardia, skin rash, weight loss, blurred vision (< 10%)
• Central nervous system: headache, insomnia, drowsiness (>10%)
• Gastrointestinal: nausea, poor appetite, dry mouth, abdominal pain (>10%)
• Risk of suicidal behaviour, hepatotoxicity
• Sedation
• Risk of cardiotoxicity
• Increased appetite
• Weight gain
• Metabolic disturbances
PHARMACOLOGICAL TREATMENT
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 9

J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 1 0
LAPORAN MAJLIS SAMBUTAN HARI RAYA JABATAN FARMASI DAN HARI LAHIR APRIL-JUN 2018
Oleh Monishah Mohanan Pillai
Jawatankuasa Kebajikan dan Sosial Jabatan Farmasi telah menganjurkan Majlis Sam-butan Hari Raya dan Sambutan Hari Lahir untuk bulan April, Mei dan Jun pada 28 Jun 2018. Sambutan ini bertujuan untuk meraikan staf yang beragama Islam di Jabatan Farmasi yang menyambut Hari Raya Aidilfitri dan juga meraikan hari lahir staf yang lahir antara bulan April sehingga bulan Jun. Dengan adanya sambutan sebegini, warga Jabatan Farmasi dapat ber-kongsi merayakan perayaan ini bersama dengan anggota jabatan lain sekaligus mengeratkan silaturrahim di kalangan anggota di HSAJB. Majlis dimulakan pada jam 11.45 pagi, dimulakan dengan bacaan doa dan disusuli dengan ucapan daripada Penaung Jawatankuasa Kebajikan dan Sosial Jabatan Farmasi, Pn Hjh Rohayah Abd Ghani. Selepas itu, majlis dimeriahkan lagi dengan acara memotong kek bagi staf yang lahir pada bulan April, Mei, dan Jun. Mereka yang terlibat telah menerima cenderahati sumbangan ikhlas daripada pihak jawatankuasa. Tidak lupa juga penyampaian hadiah kepada staf yang bertukar ke tempat baru, staf yang telah menimang cahaya mata dan staf yang baru sahaja mendirikan rumahtangga. Majlis Hari Raya dimulakan dengan marhaban daripada anggota Jabatan Farmasi. Jamuan tengahari dihidangkan dan disertai oleh Timbalan Pengarah Hospital, Ketua-Ketua Jabatan dan juga staf-staf lain daripada pelbagai jabatan. Pelbagai juadah enak disediakan untuk para tetamu menjamu selera. Secara keseluruhannya, sambutan Hari Raya Jabatan Farmasi telah berjalan dengan lancar dan meriah.