koperasi cuepacs etiqa mutiara plus wisma koperasi …kcemplus.com/claim-new/stroke/borang tuntutan...
TRANSCRIPT
KOPERASI CUEPACS ETIQA MUTIARA PLUS
Wisma Koperasi Cuepacs, No.24-4, Jln 15/48A, Sentul Raya
Boulevard, 51000 Kuala Lumpur.
Tel : 03-40440817/03-40429476 Faks : 03-40429475
Pastikan document disahkan benar lengkap mengikut arahan sebelum dihantar agar tidak berlaku
penolakan.
PERKARA: BORANG PENYAKIT KRITIKAL
NOTA : Nama Penuh Peserta merujuk kepada PESAKIT
Sijil penyertaan TKM0578/ TTMW31. Jika tiada tetapi menjadi ahli melebihi 60 hari peserta layak
membuat tuntutan. Sila lampirkan surat pengakuan jika tiada sijil.
---------------------------------------------------------------------------------------------------------------------------
Dokumen yang perlu dilampirkan:
Sila sertakan dokumen-dokumen berikut bersama dengan tuntutan ini (Salinan Disahkan) :
TYPES OF CLAIMS DOCUMENTS REQUIRED
Critical Illness
1) Borang tuntutan Penyakit Kritikal
2) Salinan Kad Pengenalan yang disahkan
3) Laporan perubatan – Penyakit Kritikal (Strok /
Jantung / ESRF / Kanser / Lain-lain) yang dilengkapi
oleh doktor
4) Sijil Asal / Salinan Sijil Penyertaan
5) Borang kebenaran untuk maklumat lanjut
6) Lain-lain dokumen yang berkenaan.
( Sila rujuk senarai dokumen sokongan bagi
tuntutan penyakit kritikal yang berkenaan)
Jika dokumen sokongan diberikan dalam salinan, dokumen tersebut mestilah disahkan oleh mereka
yang dibenarkan oleh Syarikat, Pesuruhjaya Sumpah, ‘Notary Public’, Peguam, Jaksa Pendamai,
Ahli Parlimen, Ketua Balai Polis, Penghulu atau Pegawai Daerah.
**PERMOHONAN HENDAKLAH DIPOSKAN MENGIKUT ALAMAT KAMI DI KOPERASI
CUEPACS DAN PERMOHONAN INI TIDAK BOLEH DIFAKSKAN KEPADA KAMI**
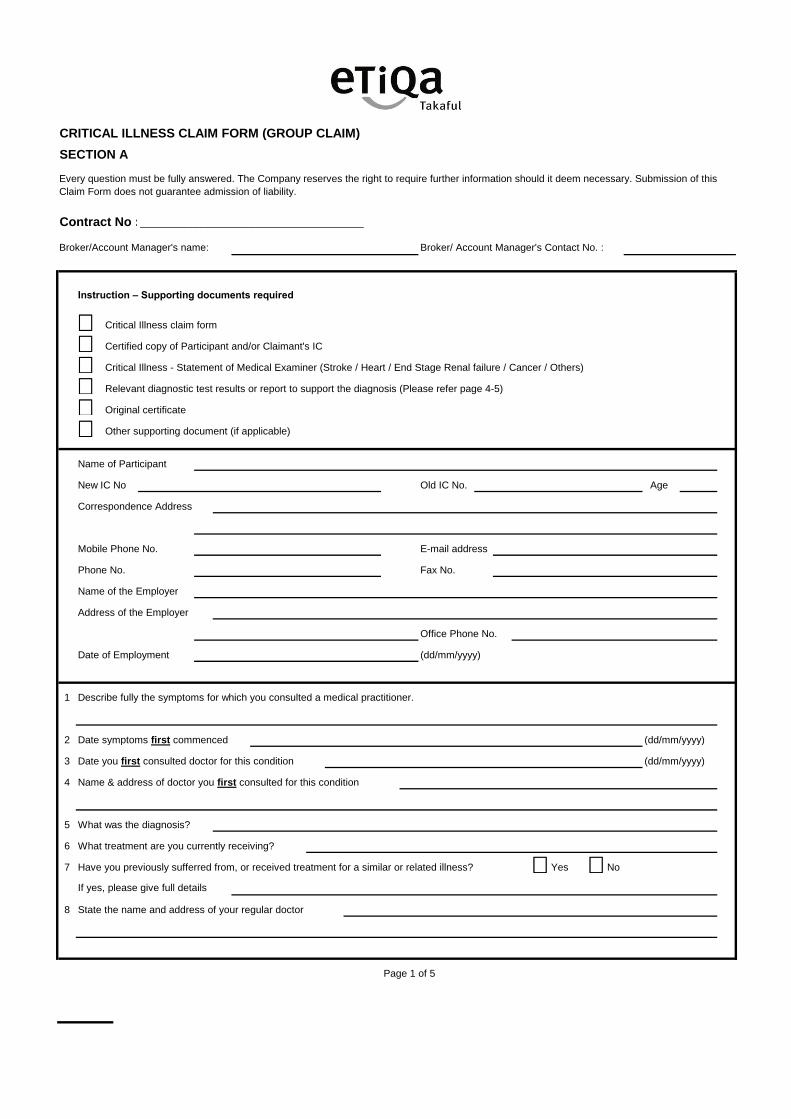
CRITICAL ILLNESS CLAIM FORM (GROUP CLAIM)
SECTION A
Contract No :________________________________________
Broker/Account Manager's name: Broker/ Account Manager's Contact No. :
Instruction – Supporting documents required
Critical Illness claim form
Certified copy of Participant and/or Claimant's IC
Critical Illness - Statement of Medical Examiner (Stroke / Heart / End Stage Renal failure / Cancer / Others)
Relevant diagnostic test results or report to support the diagnosis (Please refer page 4-5)
Original certificate
Other supporting document (if applicable)
Name of Participant
New IC No Old IC No. Age
Correspondence Address
Mobile Phone No. E-mail address
Phone No. Fax No.
Name of the Employer
Address of the Employer
Office Phone No.
Date of Employment (dd/mm/yyyy)
1 Describe fully the symptoms for which you consulted a medical practitioner.
2 Date symptoms first commenced (dd/mm/yyyy)
3 Date you first consulted doctor for this condition (dd/mm/yyyy)
4 Name & address of doctor you first consulted for this condition
5 What was the diagnosis?
6 What treatment are you currently receiving?
7 Have you previously sufferred from, or received treatment for a similar or related illness? Yes No
If yes, please give full details
8 State the name and address of your regular doctor
Page 1 of 5
Every question must be fully answered. The Company reserves the right to require further information should it deem necessary. Submission of this
Claim Form does not guarantee admission of liability.
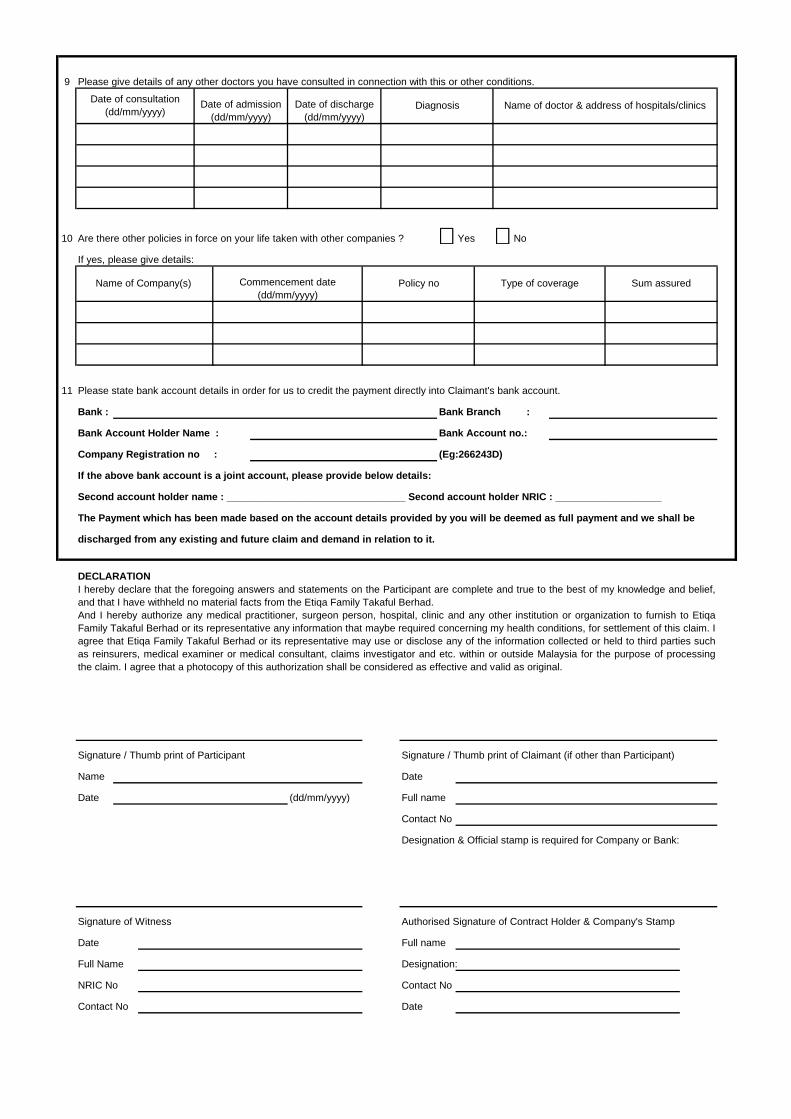
9 Please give details of any other doctors you have consulted in connection with this or other conditions.
10 Are there other policies in force on your life taken with other companies ? Yes No
If yes, please give details:
11 Please state bank account details in order for us to credit the payment directly into Claimant's bank account.
Bank : Bank Branch :
Bank Account Holder Name : Bank Account no.:
Company Registration no : (Eg:266243D)
If the above bank account is a joint account, please provide below details:
Second account holder name : ________________________________ Second account holder NRIC : ___________________
The Payment which has been made based on the account details provided by you will be deemed as full payment and we shall be
discharged from any existing and future claim and demand in relation to it.
DECLARATION
Signature / Thumb print of Participant Signature / Thumb print of Claimant (if other than Participant)
Name Date
Date (dd/mm/yyyy) Full name
Contact No
Designation & Official stamp is required for Company or Bank:
Signature of Witness Authorised Signature of Contract Holder & Company's Stamp
Date Full name
Full Name Designation:
NRIC No Contact No
Contact No Date
Date of consultation
(dd/mm/yyyy)Date of admission
(dd/mm/yyyy)
Sum assuredName of Company(s)
Date of discharge
(dd/mm/yyyy)
Policy no Type of coverageCommencement date
(dd/mm/yyyy)
Diagnosis Name of doctor & address of hospitals/clinics
I hereby declare that the foregoing answers and statements on the Participant are complete and true to the best of my knowledge and belief,
and that I have withheld no material facts from the Etiqa Family Takaful Berhad.
And I hereby authorize any medical practitioner, surgeon person, hospital, clinic and any other institution or organization to furnish to Etiqa
Family Takaful Berhad or its representative any information that maybe required concerning my health conditions, for settlement of this claim. I
agree that Etiqa Family Takaful Berhad or its representative may use or disclose any of the information collected or held to third parties such
as reinsurers, medical examiner or medical consultant, claims investigator and etc. within or outside Malaysia for the purpose of processing
the claim. I agree that a photocopy of this authorization shall be considered as effective and valid as original.
Page 2 of 5
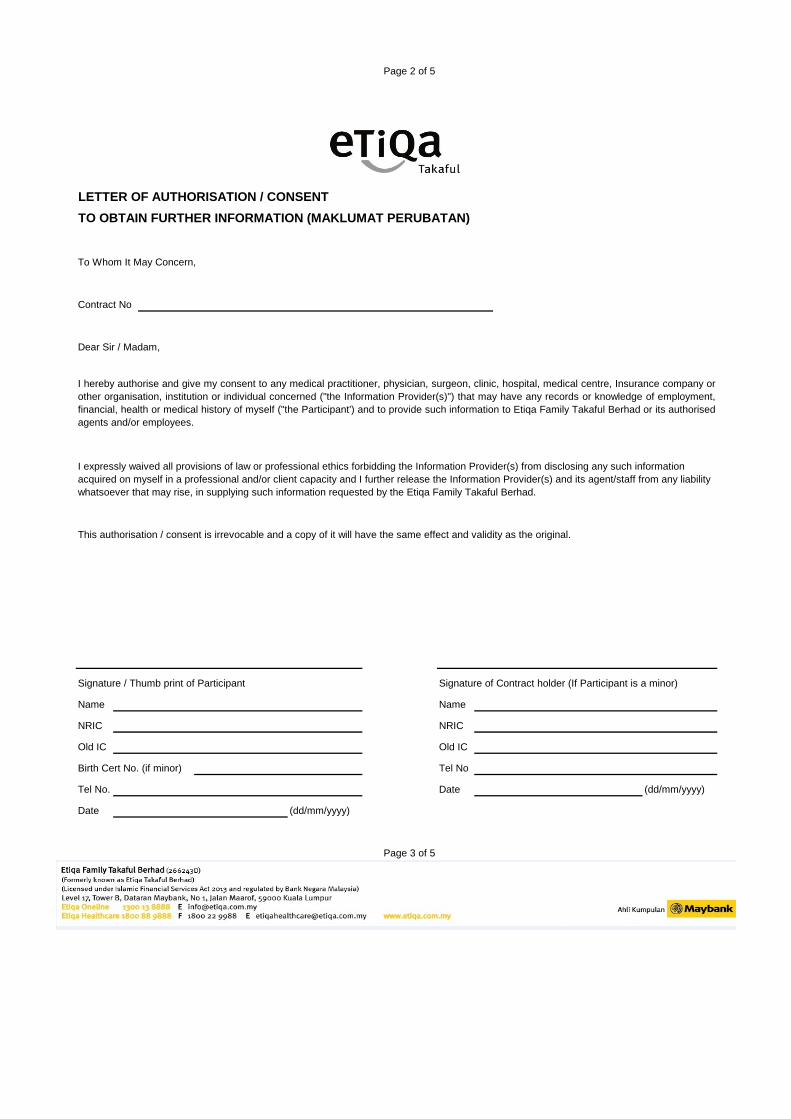
LETTER OF AUTHORISATION / CONSENT
TO OBTAIN FURTHER INFORMATION (MAKLUMAT PERUBATAN)
To Whom It May Concern,
Contract No
Dear Sir / Madam,
This authorisation / consent is irrevocable and a copy of it will have the same effect and validity as the original.
Signature / Thumb print of Participant Signature of Contract holder (If Participant is a minor)
Name Name
NRIC NRIC
Old IC Old IC
Birth Cert No. (if minor) Tel No
Tel No. Date (dd/mm/yyyy)
Date (dd/mm/yyyy)
Page 3 of 5
I expressly waived all provisions of law or professional ethics forbidding the Information Provider(s) from disclosing any such information
acquired on myself in a professional and/or client capacity and I further release the Information Provider(s) and its agent/staff from any liability
whatsoever that may rise, in supplying such information requested by the Etiqa Family Takaful Berhad.
I hereby authorise and give my consent to any medical practitioner, physician, surgeon, clinic, hospital, medical centre, Insurance company or
other organisation, institution or individual concerned ("the Information Provider(s)") that may have any records or knowledge of employment,
financial, health or medical history of myself ("the Participant') and to provide such information to Etiqa Family Takaful Berhad or its authorised
agents and/or employees.
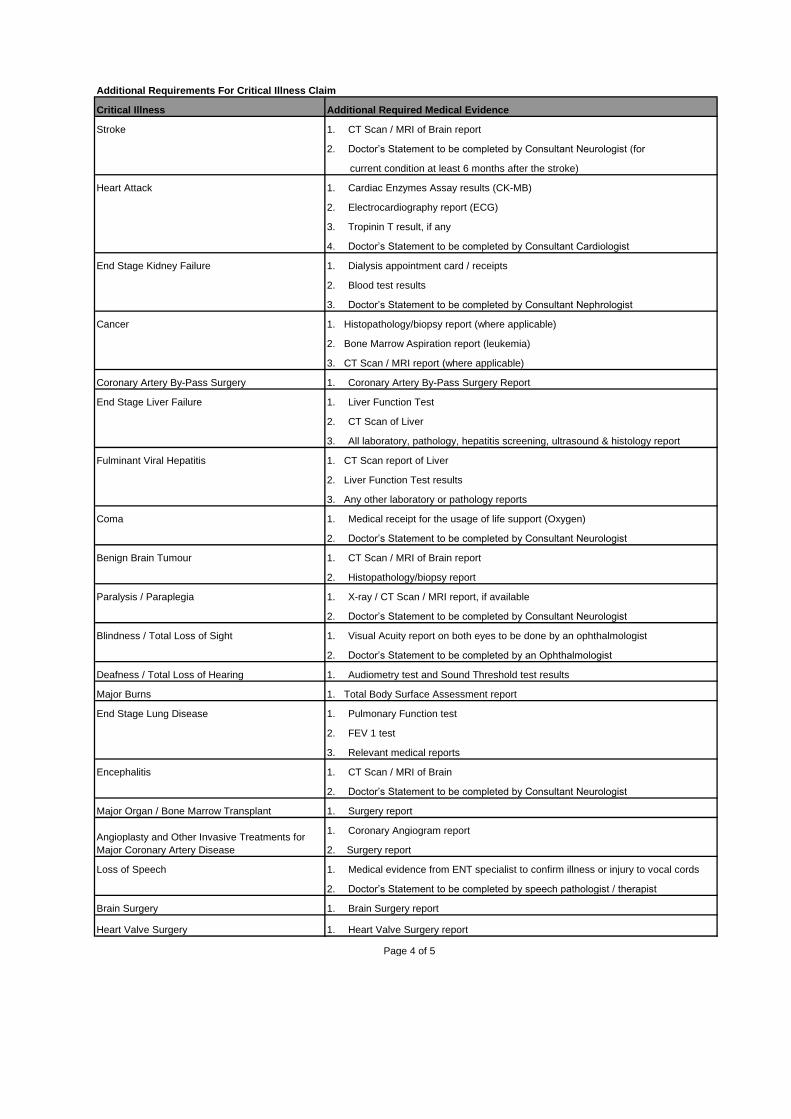
Additional Requirements For Critical Illness Claim
Critical Illness Additional Required Medical Evidence
Stroke
Heart Attack
End Stage Kidney Failure
Cancer
Coronary Artery By-Pass Surgery
End Stage Liver Failure
Fulminant Viral Hepatitis
Coma
Benign Brain Tumour
Paralysis / Paraplegia
Blindness / Total Loss of Sight
Deafness / Total Loss of Hearing
Major Burns 1. Total Body Surface Assessment report
End Stage Lung Disease
Encephalitis
Major Organ / Bone Marrow Transplant
Loss of Speech
2. Doctor’s Statement to be completed by speech pathologist / therapist
Brain Surgery
Heart Valve Surgery
Page 4 of 5
Angioplasty and Other Invasive Treatments for
Major Coronary Artery Disease
1. Brain Surgery report
1. Heart Valve Surgery report
2. FEV 1 test
1. Medical evidence from ENT specialist to confirm illness or injury to vocal cords
1. Coronary Angiogram report
3. Relevant medical reports
1. CT Scan / MRI of Brain
2. Doctor’s Statement to be completed by Consultant Neurologist
1. Surgery report
2. Surgery report
1. Visual Acuity report on both eyes to be done by an ophthalmologist
2. Doctor’s Statement to be completed by an Ophthalmologist
1. Audiometry test and Sound Threshold test results
1. Pulmonary Function test
1. X-ray / CT Scan / MRI report, if available
2. Doctor’s Statement to be completed by Consultant Neurologist
2. CT Scan of Liver
3. All laboratory, pathology, hepatitis screening, ultrasound & histology report
1. CT Scan report of Liver
2. Liver Function Test results
3. Any other laboratory or pathology reports
1. Medical receipt for the usage of life support (Oxygen)
2. Doctor’s Statement to be completed by Consultant Neurologist
1. CT Scan / MRI of Brain report
2. Histopathology/biopsy report
3. Doctor’s Statement to be completed by Consultant Nephrologist
1. Histopathology/biopsy report (where applicable)
2. Bone Marrow Aspiration report (leukemia)
3. CT Scan / MRI report (where applicable)
1. Coronary Artery By-Pass Surgery Report
1. Liver Function Test
2. Blood test results
2. Electrocardiography report (ECG)
3. Tropinin T result, if any
4. Doctor’s Statement to be completed by Consultant Cardiologist
current condition at least 6 months after the stroke)
1. CT Scan / MRI of Brain report
1. Dialysis appointment card / receipts
1. Cardiac Enzymes Assay results (CK-MB)
2. Doctor’s Statement to be completed by Consultant Neurologist (for
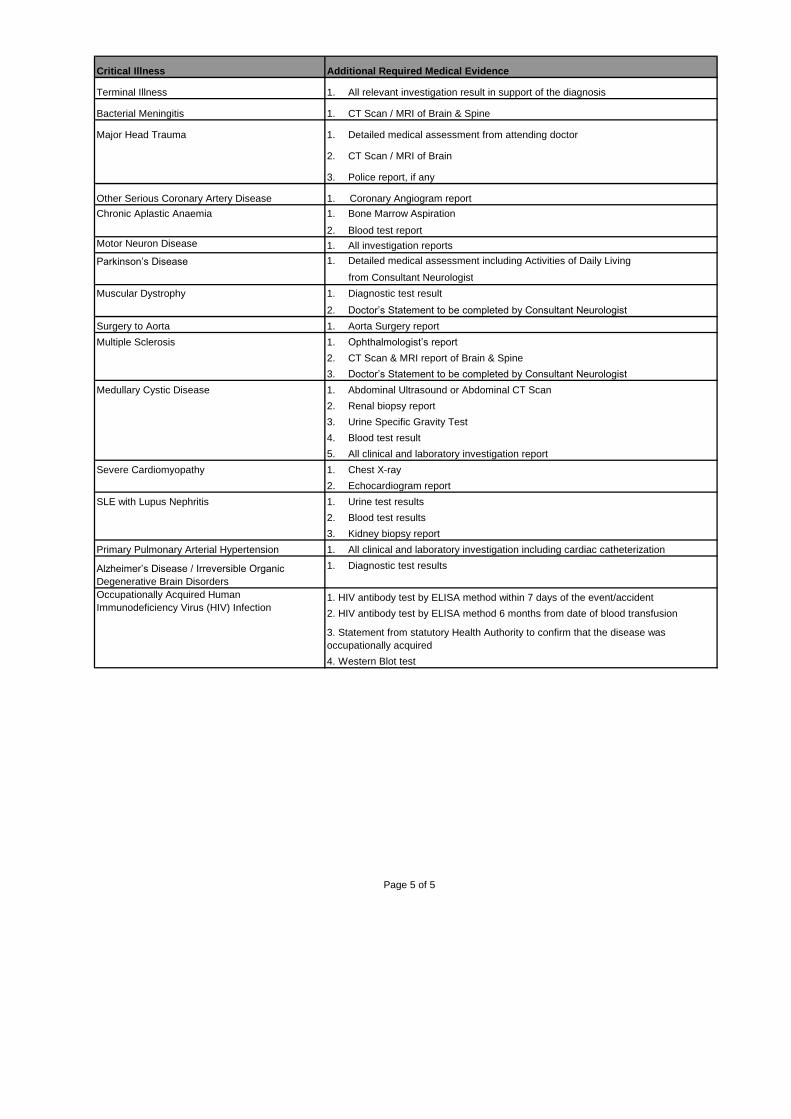
Critical Illness Additional Required Medical Evidence
Bacterial Meningitis
Major Head Trauma
Other Serious Coronary Artery Disease
Chronic Aplastic Anaemia
Parkinson’s Disease 1. Detailed medical assessment including Activities of Daily Living
from Consultant Neurologist
Surgery to Aorta
Multiple Sclerosis
Medullary Cystic Disease
SLE with Lupus Nephritis
Primary Pulmonary Arterial Hypertension
1. HIV antibody test by ELISA method within 7 days of the event/accident
2. HIV antibody test by ELISA method 6 months from date of blood transfusion
4. Western Blot test
Page 5 of 5
Alzheimer’s Disease / Irreversible Organic
Degenerative Brain Disorders
1. Diagnostic test results
2. Renal biopsy report
3. Urine Specific Gravity Test
4. Blood test result
5. All clinical and laboratory investigation report
1. Chest X-ray
2. Echocardiogram report
Severe Cardiomyopathy
1. All clinical and laboratory investigation including cardiac catheterization
1. All relevant investigation result in support of the diagnosis
1. Abdominal Ultrasound or Abdominal CT Scan
Terminal Illness
Motor Neuron Disease
Muscular Dystrophy
2. CT Scan & MRI report of Brain & Spine
2. Blood test report
1. All investigation reports
2. CT Scan / MRI of Brain
1. Bone Marrow Aspiration
1. Detailed medical assessment from attending doctor
1. Coronary Angiogram report
3. Kidney biopsy report
2. Blood test results
1. Diagnostic test result
2. Doctor’s Statement to be completed by Consultant Neurologist
3. Doctor’s Statement to be completed by Consultant Neurologist
1. Aorta Surgery report
1. Ophthalmologist’s report
1. Urine test results
3. Police report, if any
1. CT Scan / MRI of Brain & Spine
Occupationally Acquired Human
Immunodeficiency Virus (HIV) Infection
3. Statement from statutory Health Authority to confirm that the disease was
occupationally acquired
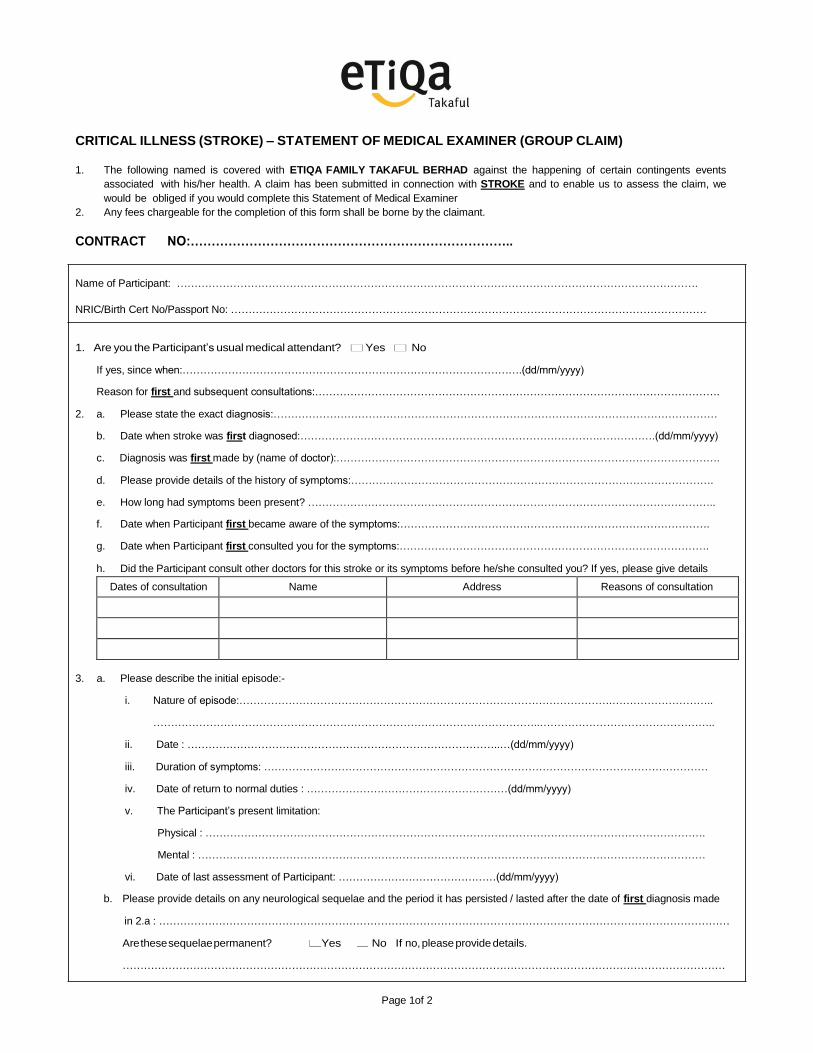
CRITICAL ILLNESS (STROKE) – STATEMENT OF MEDICAL EXAMINER (GROUP CLAIM)
1. The following named is covered with ETIQA FAMILY TAKAFUL BERHAD against the happening of certain contingents events
associated with his/her health. A claim has been submitted in connection with STROKE and to enable us to assess the claim, we
would be obliged if you would complete this Statement of Medical Examiner
2. Any fees chargeable for the completion of this form shall be borne by the claimant.
CONTRACT NO:…………………………………………………………………..
Name of Participant: ………………………………………………………………………………………………………………………………….
NRIC/Birth Cert No/Passport No: ………………………………………………………………………………………………………………………
1. Are you the Participant’s usual medical attendant? Yes No
If yes, since when:…………………………………………………………………………………….(dd/mm/yyyy)
Reason for first and subsequent consultations:…………………………………………………………………………………………………….
2. a. Please state the exact diagnosis:………………………………………………………………………………………………………………
b. Date when stroke was first diagnosed:………………………………………………………………………….…………….(dd/mm/yyyy)
c. Diagnosis was first made by (name of doctor):……………………………………………………………………………………………….
d. Please provide details of the history of symptoms:………………………………………………………………………………………….
e. How long had symptoms been present? ……………………………………………………………………………………………………..
f. Date when Participant first became aware of the symptoms:…………………………………………………………………………….
g. Date when Participant first consulted you for the symptoms:…………………………………………………………………………….
h. Did the Participant consult other doctors for this stroke or its symptoms before he/she consulted you? If yes, please give details
Dates of consultation Name Address Reasons of consultation
3. a. Please describe the initial episode:-
i. Nature of episode:…………………………………………………………………………………………….………………………..
………………………………………………………………………………………………..…………………………………………..
ii. Date : ……………………………………………………………………………..…(dd/mm/yyyy)
iii. Duration of symptoms: ………………………………………………………………………………………………………………
iv. Date of return to normal duties : …………………………………………………(dd/mm/yyyy)
v. The Participant’s present limitation:
Physical : …………………………………………………………………………………………………………………………….
Mental : ………………………………………………………………………………………………………………………………
vi. Date of last assessment of Participant: ………………………………………(dd/mm/yyyy)
b. Please provide details on any neurological sequelae and the period it has persisted / lasted after the date of first diagnosis made
in 2.a : ………………………………………………………………………………………………………………………………………………
Are these sequelae permanent? Yes No If no, please provide details.
………………………………………………………………………………………………………………………………………………………
Page 1of 2
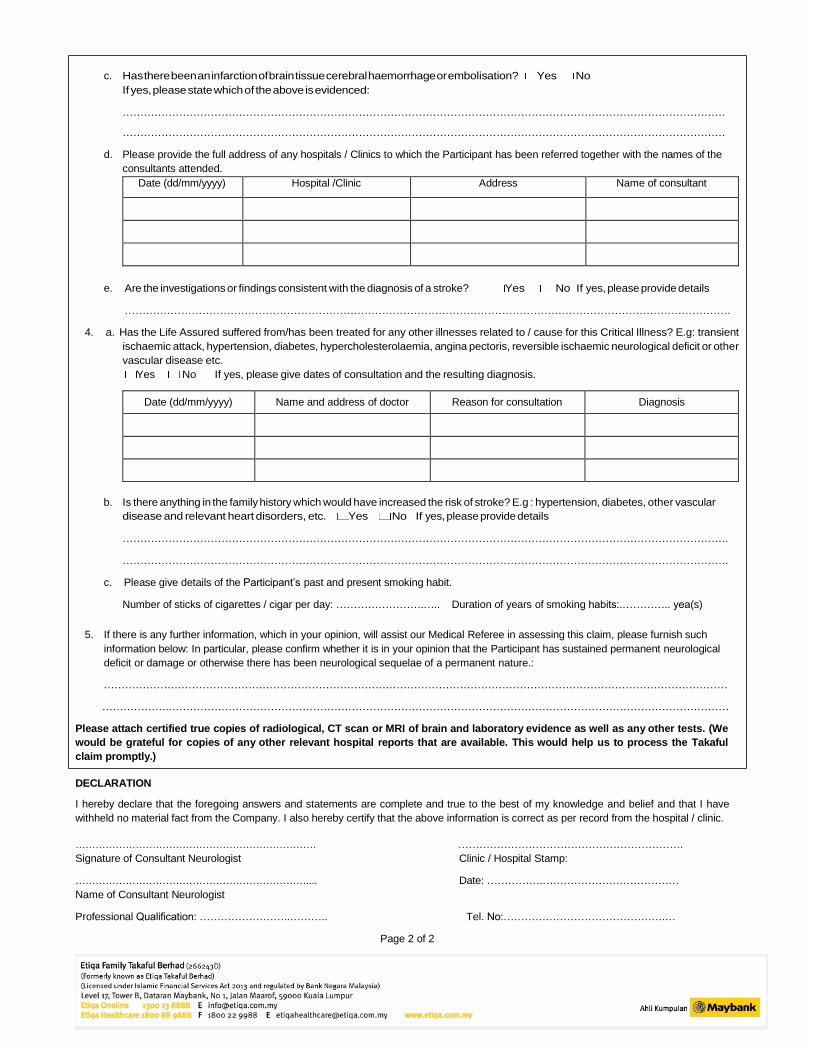
c. Has there been an infarction of brain tissue cerebral haemorrhage or embolisation? Yes No
If yes, please state which of the above is evidenced:
………………………………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………………………………
d. Please provide the full address of any hospitals / Clinics to which the Participant has been referred together with the names of the
consultants attended.
Date (dd/mm/yyyy) Hospital /Clinic Address Name of consultant
e. Are the investigations or findings consistent with the diagnosis of a stroke? Yes No If yes, please provide details
……………………………………………………………………………………………………………………………………………………….
4. a. Has the Life Assured suffered from/has been treated for any other illnesses related to / cause for this Critical Illness? E.g: transient
ischaemic attack, hypertension, diabetes, hypercholesterolaemia, angina pectoris, reversible ischaemic neurological deficit or other
vascular disease etc.
Yes No If yes, please give dates of consultation and the resulting diagnosis.
Date (dd/mm/yyyy) Name and address of doctor Reason for consultation Diagnosis
b. Is there anything in the family history which would have increased the risk of stroke? E.g : hypertension, diabetes, other vascular
disease and relevant heart disorders, etc. Yes No If yes, please provide details
……………………………………………………………………………………………………………………………………………………….
……………………………………………………………………………………………………………………………………………………….
c. Please give details of the Participant’s past and present smoking habit.
Number of sticks of cigarettes / cigar per day: …………………….….. Duration of years of smoking habits:.………….. yea(s)
5. If there is any further information, which in your opinion, will assist our Medical Referee in assessing this claim, please furnish such
information below: In particular, please confirm whether it is in your opinion that the Participant has sustained permanent neurological
deficit or damage or otherwise there has been neurological sequelae of a permanent nature.:
……………………………………………………………………………………………………………………………………………………………
……………….……………………………………………………………………………………………………………………………………………
Please attach certified true copies of radiological, CT scan or MRI of brain and laboratory evidence as well as any other tests. (We
would be grateful for copies of any other relevant hospital reports that are available. This would help us to process the Takaful
claim promptly.)
DECLARATION
I hereby declare that the foregoing answers and statements are complete and true to the best of my knowledge and belief and that I have
withheld no material fact from the Company. I also hereby certify that the above information is correct as per record from the hospital / clinic.
……………………………………………………………… ……………………………………………………….
Signature of Consultant Neurologist Clinic / Hospital Stamp:
…………………………………………………………….... Date: …………….…………………………………
Name of Consultant Neurologist
Professional Qualification: ……………………..……….. Tel. No:……………………………………….…
Page 2 of 2