eagle's syndrome - e-mjm.org · should be performed to confirm the diagnosis. analgesics and...
TRANSCRIPT
CASE REPORT
Eagle's Syndrome
IF m
S Subramaniam, MS (ORL)*, M D Abd Majid, MS (ORL)**
*Faculty of Medicine and Health Sciences, University Putra Malaysia, 43400 Serdang, Kuala Lumpur, ** Departmentof Otorhinolaryngology, Hospital Kuala Lumpur, Jalan Pahang 50586 Kuala Lumpur
Introduction
Eagle' Syndrome is an uncommon disease whichmay cause Cervico facial pain and tinnitus3• It wasfirst described in 1937 by W. W. Eagle. Symptoms,physical signs, theories of causation and currenttreatment are discussed.
Case Report
A 48 years female presented to theOtolaryngology clinic of Hospital Kuala Lumpurwith a one-year history of bilateral upper neckpain especially during yawning and mouthopening. There was associated tinnitus andreferred otalgia. There was no history of hearingloss. On examination of oropahrynx, both tonsilswere found to be atrophic and on deep palpation
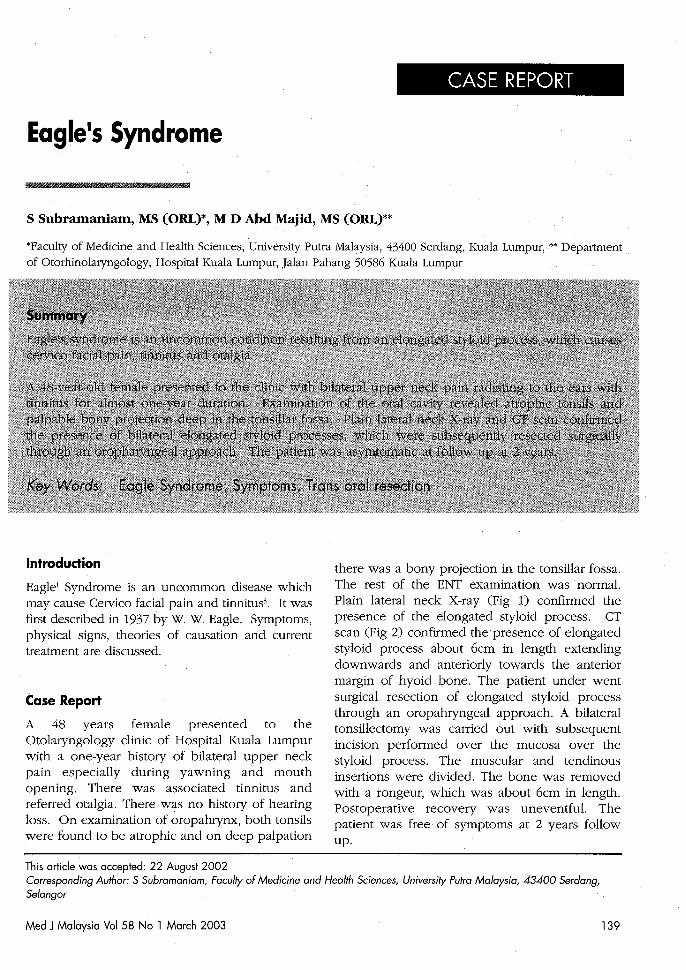
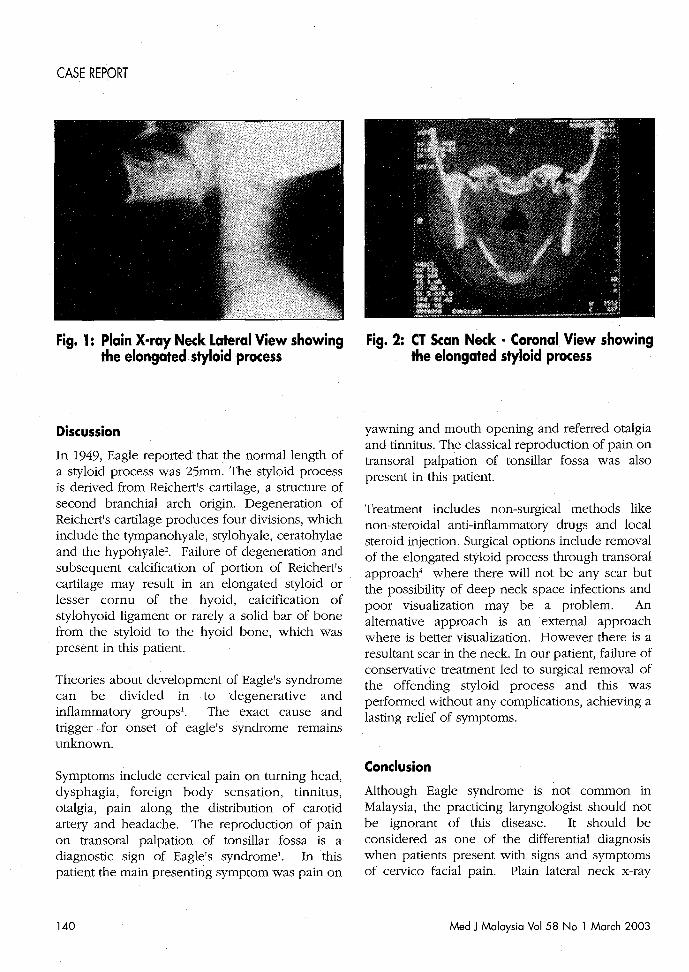
there was a bony projection in the tonsillar fossa.The rest of the ENT examination was normal.Plain lateral neck X-ray (Fig 1) confirmed thepresence of the elongated styloid process. CTscan (Fig 2) confirmed the presence of elongatedstyloid process about 6cm in length extendingdownwards and anteriorly towards the anteriormargin of hyoid bone. The patient under wentsurgical resection of elongated styloid processthrough an oropahryngeal approach. A bilateraltonsillectomy was carried out with subsequentincision performed over the mucosa over thestyloid process. The muscular and tendinousinsertions were divided. The bone was removedwith a rongeur, which was about 6cm in length.Postoperative recovery was uneventful. Thepatient was free of symptoms at 2 years followup.
This article was accepted: 22 August 2002Corresponding Author: S Subramaniam, Faculty of Medicine and Health Sciences, University Putra Malaysia, 43400 Serdang,Selangor
Med J Malaysia Vol 58 No 1 March 2003 139
CASE REPORT
Fig. 1: Plain X-ray Neck Lateral View showingthe elongated styloid process
Discussion
In 1949, Eagle reported that the normal length ofa styloid process was 25mm. The styloid processis derived from Reichert's cartilage, a structure ofsecond branchial arch origin. Degeneration ofReichert's cartilage produces four divisions, whichinclude the tympanohyale, stylohyale, ceratohylaeand the hypohyalez. Failure of degeneration andsubsequent calcification of portion of Reichert'scartilage may result in an elongated stylOid orlesser cornu of the hyoid, calcification ofstylohyoid ligament or rarely a solid bar of bonefrom the stylOid to the hyoid bone, which waspresent in this patient.
Theories about development of Eagle's syndromecan be divided in to degenerative andinflammatory groups'. The exact cause andtrigger .·for onset of eagle's syndrome remainsunknown.
Symptoms include cervical pain on turning head,dysphagia, foreign body sensation, tinnitus,otalgia, pain along the distribution of carotidartery and headache. The reproduction of painon transoral palpation of tonsillar fossa is adiagnostic sign of Eagle's syndrome'. In thispatient the main presenting symptom was pain on
140
Fig. 2: CT Scan Neck - Coronal View showingthe elongated styloid process
yawning and mouth opening and referred otalgiaand tinnitus. The classical reproduction of pain ontransoral palpation of tonsillar fossa was alsopresent in this patient.
Treatment includes non-surgical methods likenon-steroidal anti-inflammatory drugs and localsteroid injection. Surgical options include removalof the elongated styloid process through transoralapproach4 where there will not be any scar butthe possibility of deep neck space infections andpoor visualization may be a problem. Analternative approach is an external approachwhere is better visualization. However there is aresultant scar in the neck. In our patient, failure ofconservative treatment led to surgical removal ofthe offending styloid process and this wasperformed without any complications, achieving alasting relief of symptoms.
Conclusion
Although Eagle syndrome is not common inMalaysia, the practicing laryngologist should notbe ignorant of this disease. It should beconsidered as one of the differential diagnosiswhen patients present with signs and symptomsof cervico facial pain. Plain lateral neck x-ray
Med J Malaysia Vol 58 No 1 March 2003
should be performed to confirm the diagnosis.Analgesics and anti-inflammatory medication maybe helpful. Surgical resection of elongated styloid
Eagle's Syndrome
process is indicated with the failure ofconservative treatment.
'"111 lilll 1111 II
1. Baugh RF, Rose Mary Stocks. Eagle's Syndrome: areappraisal. Ear Nose Throat] 1993; 72(5): 341-4
2. Rechtweg ]S, Wax MK. Eagle's Syndrome: AReview. Am] Otolaryngol 1998; 19(5): 316-21.
Mad J Malaysia Vol 58 No 1 March 2003
3. Eagle WW. Elongated styloid processes: Report oftwo cases. Arch Otolaryngol 1937; 25: 584-6.
4. Strauss M, Zohar Y, laurean N. Elongated styloidprocess syndrome. Intra oral versus externalapproach for styloid surgery. Laryngoscope 1985;95: 976-9.
141