page 2 3 page vs copd 4 5 primary and secondary...
TRANSCRIPT
BU
LE
TIN
VOLUME 2/2018
MAY 2018
EDITORIAL BOARD ADVISOR: PN HJH ROHAYAH BT. ABD. GHANI EDITORS: PN SITI ROSNAH BT. SURADI EN MOHD SHAFIE BIN ZABIDI PN PATRICIA LIM MING HUA PN LI SHIN GIE
HOSPITAL SULTANAH AMINAH JOHOR BAHRU KEMENTERIAN KESIHATAN MALAYSIA JALAN PERSIARAN ABU BAKAR SULTAN 80100 JOHOR BAHRU TEL: 07-2257000 FAX: 07-2242694 EMAIL: [email protected]
IN THIS ISSUE
HEPATITIS C TREATMENT GUIDELINE
PRIMARY AND SECONDARY PREVENTION OF CARDIOVASCULAR DISEASE 2017
PAGE 2 - 3
PAGE 4 - 5
UPDATES IN MANAGEMENT OF ASTHMA VS COPD
HORMONAL THERAPY IN SUBFERTILITY
PAGE 6- 7
PAGE 8 - 9
LAPORAN AKTIVITI BERGAMBAR PAMERAN KUA BERSEMPENA HARI BUAH PINGGANG SEDUNIA 2018
PAGE 10
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 2
BY IZZATI AFIQAH JAILANI WHAT IS HEPATITIS C?
A liver disease caused by the hepatitis C virus (HCV); a blood borne virus which can cause either acute or chronic illness ranging from a mild illness lasting a few weeks to a serious, lifelong illness.
It can be transmitted through sharing of needles and syringes, reuse of contaminated syringes, sexual transmission, blood transfusion, mother to fetus and needle prick injury.
People who are HCV infected are at risk of developing advanced liver disease; 60% - 70% will develop liver cirrhosis, 1% - 5% will die of cirrhosis or hepatocellular carcinoma.
• Treatment for HCV infection differs in regime and duration by : – The status of infection
– Genotype – Complication of the disease
• The most common genotypes in Malaysia are genotype 3 (56%) and 1 (39%). Genotype 2 and 4 are the least common.
• Survival rate: Genotype 1: ~50% Genotype 2 & 3: ~80%
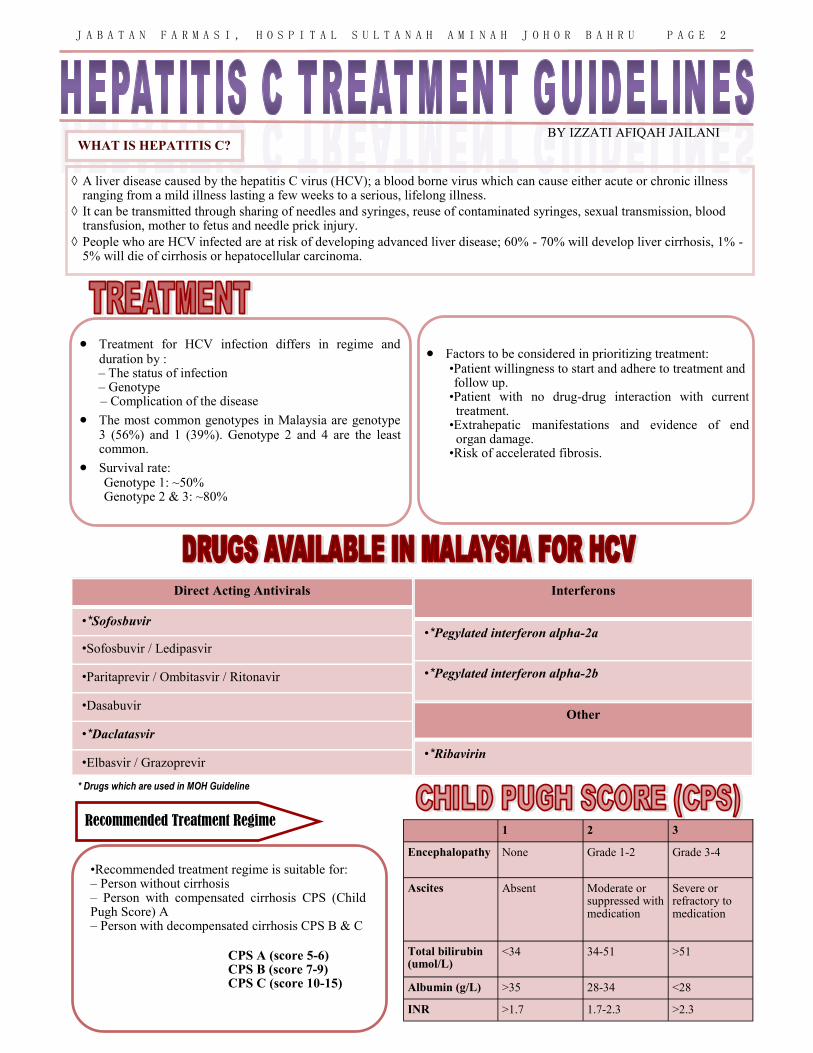
•Recommended treatment regime is suitable for: – Person without cirrhosis – Person with compensated cirrhosis CPS (Child Pugh Score) A – Person with decompensated cirrhosis CPS B & C
Recommended Treatment Regime
• Factors to be considered in prioritizing treatment: •Patient willingness to start and adhere to treatment and follow up. •Patient with no drug-drug interaction with current treatment. •Extrahepatic manifestations and evidence of end organ damage. •Risk of accelerated fibrosis.
Direct Acting Antivirals
•*Sofosbuvir
•Sofosbuvir / Ledipasvir
•Paritaprevir / Ombitasvir / Ritonavir
•Dasabuvir
•*Daclatasvir
•Elbasvir / Grazoprevir
Interferons
•*Pegylated interferon alpha-2a
•*Pegylated interferon alpha-2b
Other
•*Ribavirin
CPS A (score 5-6) CPS B (score 7-9) CPS C (score 10-15)
1 2 3
Encephalopathy None Grade 1-2 Grade 3-4
Ascites Absent Moderate or suppressed with medication
Severe or refractory to medication
Total bilirubin (umol/L)
<34 34-51 >51
Albumin (g/L) >35 28-34 <28
INR >1.7 1.7-2.3 >2.3
* Drugs which are used in MOH Guideline
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 3
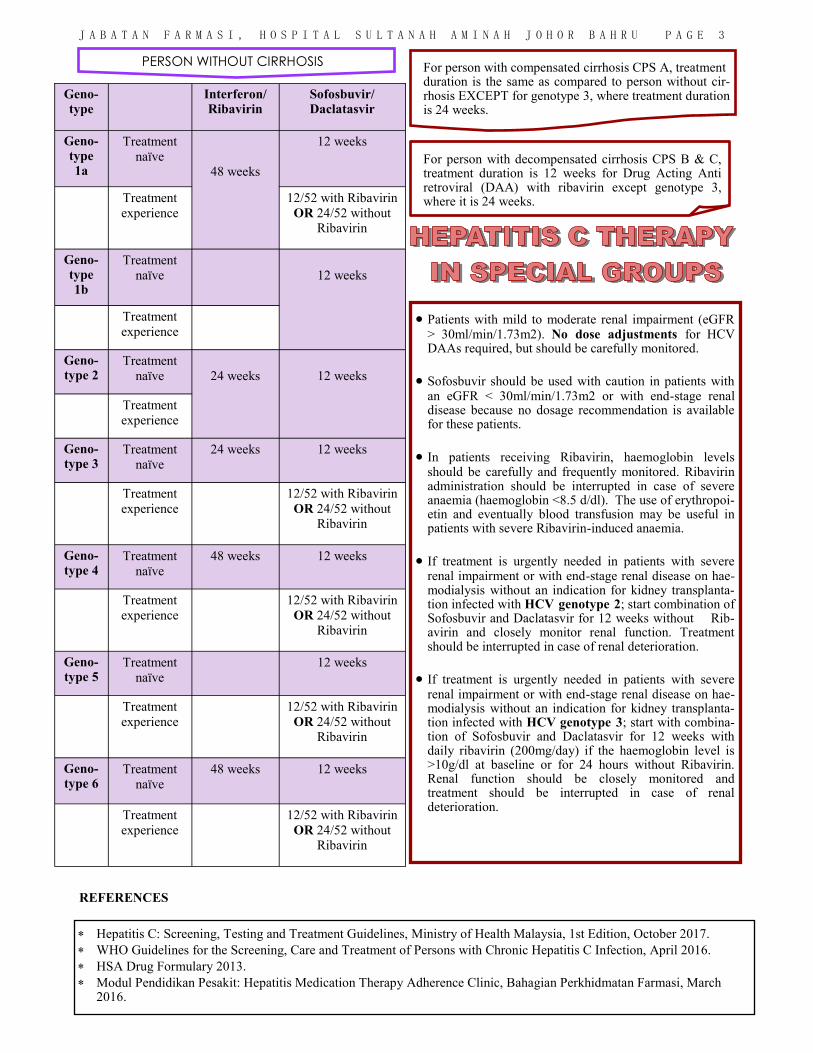
For person with compensated cirrhosis CPS A, treatment duration is the same as compared to person without cir-rhosis EXCEPT for genotype 3, where treatment duration is 24 weeks.
• Patients with mild to moderate renal impairment (eGFR > 30ml/min/1.73m2). No dose adjustments for HCV DAAs required, but should be carefully monitored.
• Sofosbuvir should be used with caution in patients with an eGFR < 30ml/min/1.73m2 or with end-stage renal disease because no dosage recommendation is available for these patients.
• In patients receiving Ribavirin, haemoglobin levels should be carefully and frequently monitored. Ribavirin administration should be interrupted in case of severe anaemia (haemoglobin <8.5 d/dl). The use of erythropoi-etin and eventually blood transfusion may be useful in patients with severe Ribavirin-induced anaemia.
• If treatment is urgently needed in patients with severe renal impairment or with end-stage renal disease on hae-modialysis without an indication for kidney transplanta-tion infected with HCV genotype 2; start combination of Sofosbuvir and Daclatasvir for 12 weeks without Rib-avirin and closely monitor renal function. Treatment should be interrupted in case of renal deterioration.
• If treatment is urgently needed in patients with severe renal impairment or with end-stage renal disease on hae-modialysis without an indication for kidney transplanta-tion infected with HCV genotype 3; start with combina-tion of Sofosbuvir and Daclatasvir for 12 weeks with daily ribavirin (200mg/day) if the haemoglobin level is >10g/dl at baseline or for 24 hours without Ribavirin. Renal function should be closely monitored and treatment should be interrupted in case of renal deterioration.
Hepatitis C: Screening, Testing and Treatment Guidelines, Ministry of Health Malaysia, 1st Edition, October 2017.
WHO Guidelines for the Screening, Care and Treatment of Persons with Chronic Hepatitis C Infection, April 2016.
HSA Drug Formulary 2013.
Modul Pendidikan Pesakit: Hepatitis Medication Therapy Adherence Clinic, Bahagian Perkhidmatan Farmasi, March 2016.
REFERENCES
PERSON WITHOUT CIRRHOSIS
Geno-
type Interferon/
Ribavirin Sofosbuvir/
Daclatasvir
Geno-
type 1a
Treatment
naïve
48 weeks
12 weeks
Treatment
experience
12/52 with Ribavirin
OR 24/52 without Ribavirin
Geno-
type 1b
Treatment
naïve
12 weeks
Treatment
experience
Geno-
type 2 Treatment
naïve
24 weeks
12 weeks
Treatment
experience
Geno-
type 3 Treatment
naïve
24 weeks 12 weeks
Treatment
experience
12/52 with Ribavirin
OR 24/52 without Ribavirin
Geno-
type 4 Treatment
naïve
48 weeks 12 weeks
Treatment
experience
12/52 with Ribavirin
OR 24/52 without Ribavirin
Geno-
type 5 Treatment
naïve
12 weeks
Treatment
experience
12/52 with Ribavirin
OR 24/52 without Ribavirin
Geno-
type 6 Treatment
naïve
48 weeks 12 weeks
Treatment
experience
12/52 with Ribavirin
OR 24/52 without Ribavirin
For person with decompensated cirrhosis CPS B & C, treatment duration is 12 weeks for Drug Acting Anti retroviral (DAA) with ribavirin except genotype 3, where it is 24 weeks.
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 4
Updates in Management of Asthma vs COPD
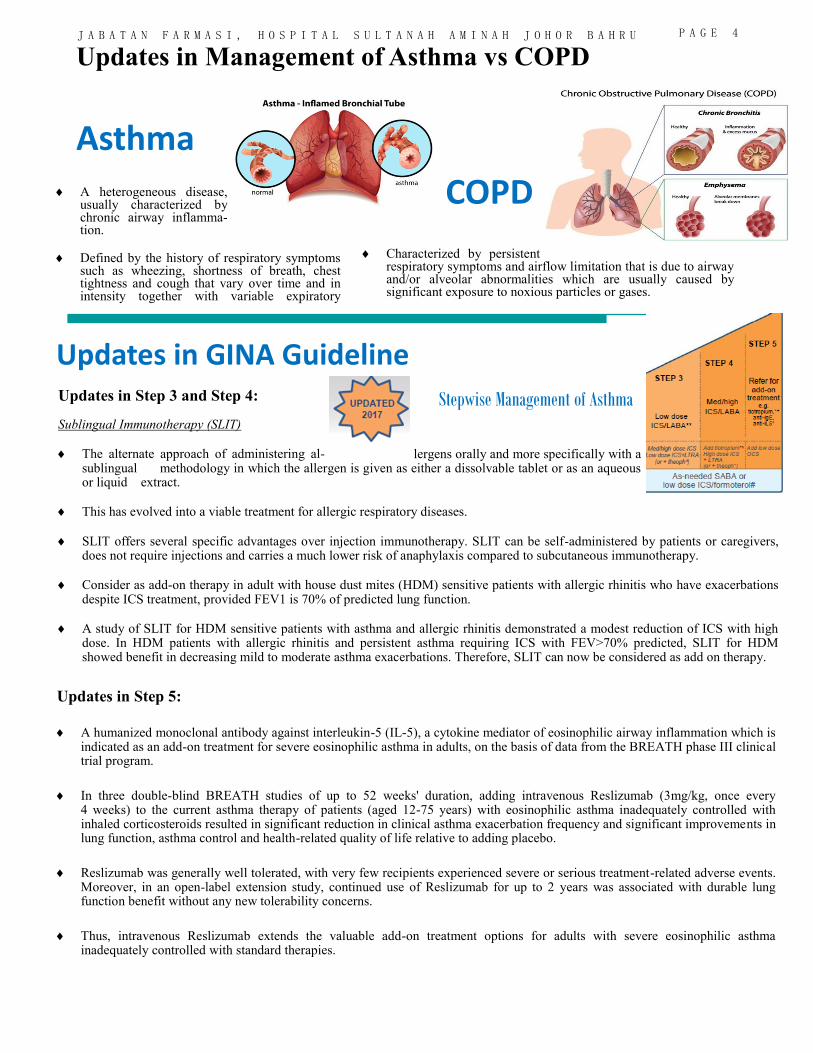
Asthma A heterogeneous disease,
usually characterized by chronic airway inflamma-tion.
Defined by the history of respiratory symptoms such as wheezing, shortness of breath, chest tightness and cough that vary over time and in intensity together with variable expiratory
Characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities which are usually caused by significant exposure to noxious particles or gases.
COPD
Updates in Step 3 and Step 4:
Sublingual Immunotherapy (SLIT)
The alternate approach of administering al- lergens orally and more specifically with a sublingual methodology in which the allergen is given as either a dissolvable tablet or as an aqueous or liquid extract.
This has evolved into a viable treatment for allergic respiratory diseases.
SLIT offers several specific advantages over injection immunotherapy. SLIT can be self-administered by patients or caregivers, does not require injections and carries a much lower risk of anaphylaxis compared to subcutaneous immunotherapy.
Consider as add-on therapy in adult with house dust mites (HDM) sensitive patients with allergic rhinitis who have exacerbations despite ICS treatment, provided FEV1 is 70% of predicted lung function.
A study of SLIT for HDM sensitive patients with asthma and allergic rhinitis demonstrated a modest reduction of ICS with high dose. In HDM patients with allergic rhinitis and persistent asthma requiring ICS with FEV>70% predicted, SLIT for HDM showed benefit in decreasing mild to moderate asthma exacerbations. Therefore, SLIT can now be considered as add on therapy.
Updates in Step 5:
A humanized monoclonal antibody against interleukin-5 (IL-5), a cytokine mediator of eosinophilic airway inflammation which is indicated as an add-on treatment for severe eosinophilic asthma in adults, on the basis of data from the BREATH phase III clinical trial program.
In three double-blind BREATH studies of up to 52 weeks' duration, adding intravenous Reslizumab (3mg/kg, once every 4 weeks) to the current asthma therapy of patients (aged 12-75 years) with eosinophilic asthma inadequately controlled with inhaled corticosteroids resulted in significant reduction in clinical asthma exacerbation frequency and significant improvements in lung function, asthma control and health-related quality of life relative to adding placebo.
Reslizumab was generally well tolerated, with very few recipients experienced severe or serious treatment-related adverse events. Moreover, in an open-label extension study, continued use of Reslizumab for up to 2 years was associated with durable lung function benefit without any new tolerability concerns.
Thus, intravenous Reslizumab extends the valuable add-on treatment options for adults with severe eosinophilic asthma inadequately controlled with standard therapies.
Updates in GINA Guideline
Stepwise Management of Asthma
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 5
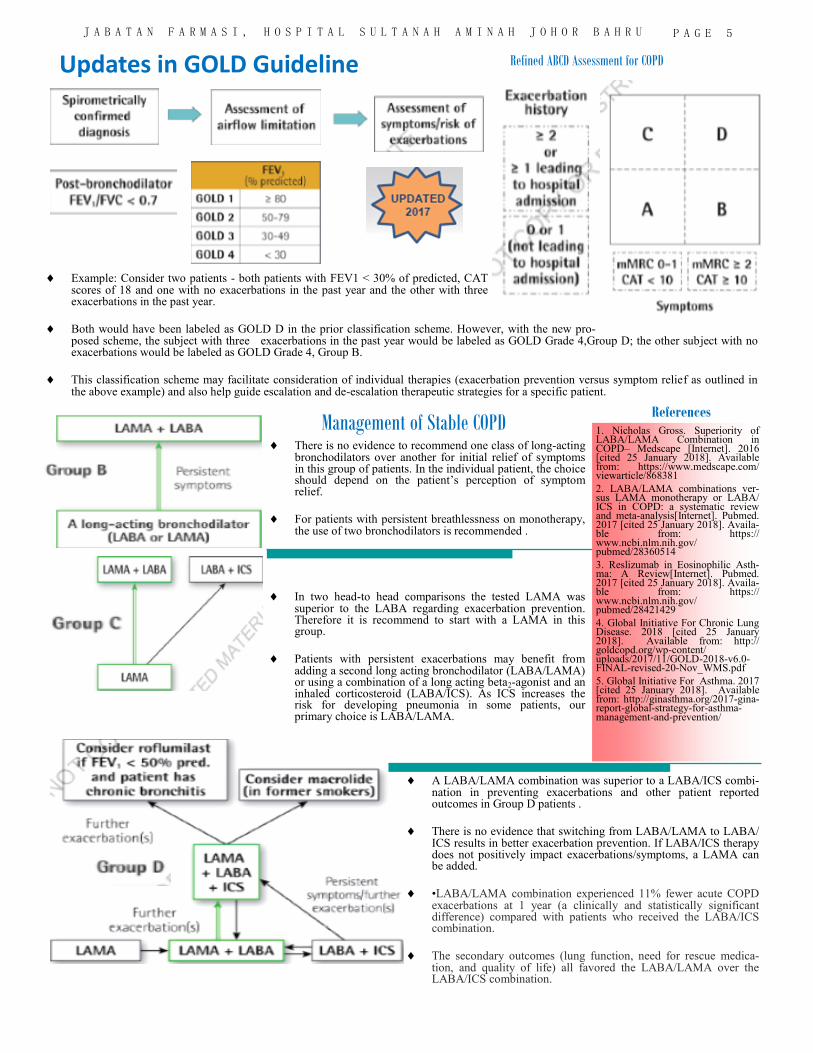
Updates in GOLD Guideline Refined ABCD Assessment for COPD
Example: Consider two patients - both patients with FEV1 < 30% of predicted, CAT scores of 18 and one with no exacerbations in the past year and the other with three exacerbations in the past year.
Both would have been labeled as GOLD D in the prior classification scheme. However, with the new pro-posed scheme, the subject with three exacerbations in the past year would be labeled as GOLD Grade 4,Group D; the other subject with no exacerbations would be labeled as GOLD Grade 4, Group B.
This classification scheme may facilitate consideration of individual therapies (exacerbation prevention versus symptom relief as outlined in the above example) and also help guide escalation and de-escalation therapeutic strategies for a specific patient.
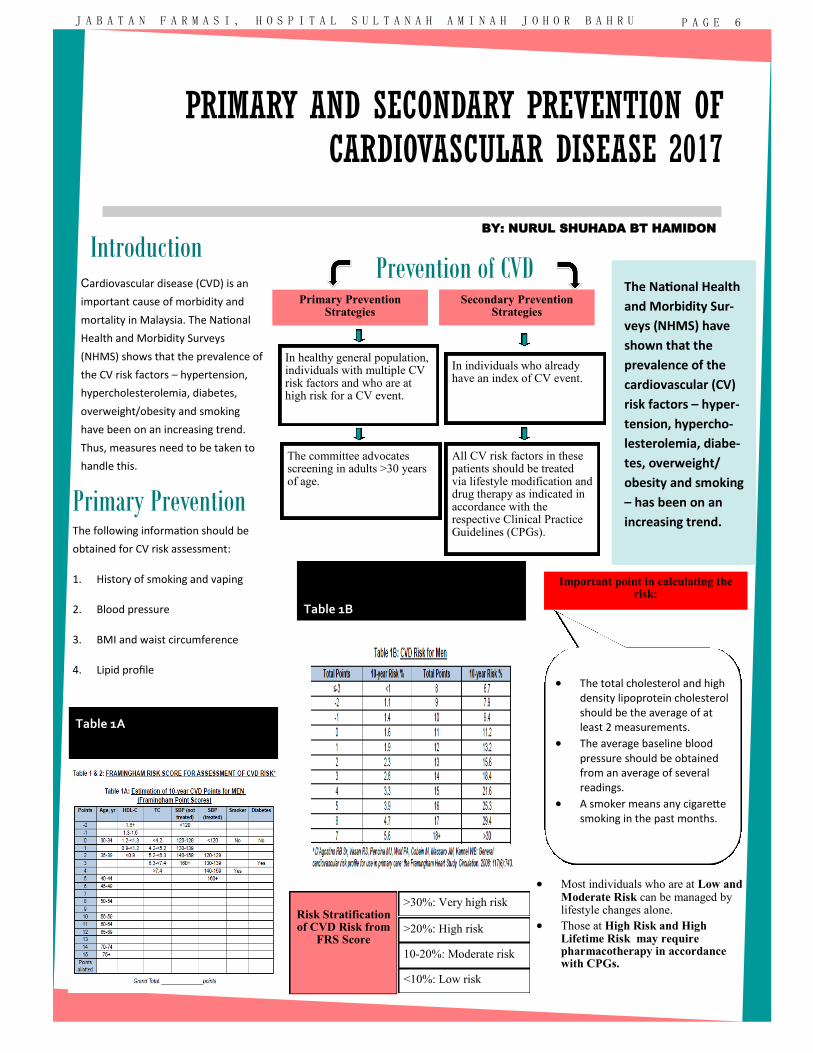
References Management of Stable COPD
There is no evidence to recommend one class of long-acting bronchodilators over another for initial relief of symptoms in this group of patients. In the individual patient, the choice should depend on the patient’s perception of symptom relief.
For patients with persistent breathlessness on monotherapy, the use of two bronchodilators is recommended .
In two head-to head comparisons the tested LAMA was superior to the LABA regarding exacerbation prevention. Therefore it is recommend to start with a LAMA in this group.
Patients with persistent exacerbations may benefit from adding a second long acting bronchodilator (LABA/LAMA) or using a combination of a long acting beta2-agonist and an inhaled corticosteroid (LABA/ICS). As ICS increases the risk for developing pneumonia in some patients, our primary choice is LABA/LAMA.
A LABA/LAMA combination was superior to a LABA/ICS combi-nation in preventing exacerbations and other patient reported outcomes in Group D patients .
There is no evidence that switching from LABA/LAMA to LABA/ICS results in better exacerbation prevention. If LABA/ICS therapy does not positively impact exacerbations/symptoms, a LAMA can be added.
•LABA/LAMA combination experienced 11% fewer acute COPD exacerbations at 1 year (a clinically and statistically significant difference) compared with patients who received the LABA/ICS combination.
The secondary outcomes (lung function, need for rescue medica-tion, and quality of life) all favored the LABA/LAMA over the LABA/ICS combination.
1. Nicholas Gross. Superiority of LABA/LAMA Combination in COPD– Medscape [Internet]. 2016 [cited 25 January 2018]. Available from: https://www.medscape.com/viewarticle/868381
2. LABA/LAMA combinations ver-sus LAMA monotherapy or LABA/ICS in COPD: a systematic review and meta-analysis[Internet]. Pubmed. 2017 [cited 25 January 2018]. Availa-ble from: https://www.ncbi.nlm.nih.gov/pubmed/28360514
3. Reslizumab in Eosinophilic Asth-ma: A Review[Internet]. Pubmed. 2017 [cited 25 January 2018]. Availa-ble from: https://www.ncbi.nlm.nih.gov/pubmed/28421429
4. Global Initiative For Chronic Lung Disease. 2018 [cited 25 January 2018]. Available from: http://goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-revised-20-Nov_WMS.pdf
5. Global Initiative For Asthma. 2017 [cited 25 January 2018]. Available from: http://ginasthma.org/2017-gina-report-global-strategy-for-asthma-management-and-prevention/
Cardiovascular disease (CVD) is an
important cause of morbidity and
mortality in Malaysia. The National
Health and Morbidity Surveys
(NHMS) shows that the prevalence of
the CV risk factors – hypertension,
hypercholesterolemia, diabetes,
overweight/obesity and smoking
have been on an increasing trend.
Thus, measures need to be taken to
handle this.
Primary Prevention Strategies
Primary Prevention The following information should be
obtained for CV risk assessment:
1. History of smoking and vaping
2. Blood pressure
3. BMI and waist circumference
4. Lipid profile
Important point in calculating the risk:
The National Health
and Morbidity Sur-
veys (NHMS) have
shown that the
prevalence of the
cardiovascular (CV)
risk factors – hyper-
tension, hypercho-
lesterolemia, diabe-
tes, overweight/
obesity and smoking
– has been on an
increasing trend.
BY: NURUL SHUHADA BT HAMIDON
Prevention of CVD
In healthy general population, individuals with multiple CV risk factors and who are at high risk for a CV event.
In individuals who already have an index of CV event.
The committee advocates screening in adults >30 years of age.
All CV risk factors in these patients should be treated via lifestyle modification and drug therapy as indicated in accordance with the respective Clinical Practice Guidelines (CPGs).
• The total cholesterol and high density lipoprotein cholesterol should be the average of at least 2 measurements.
• The average baseline blood pressure should be obtained from an average of several readings.
• A smoker means any cigarette smoking in the past months.
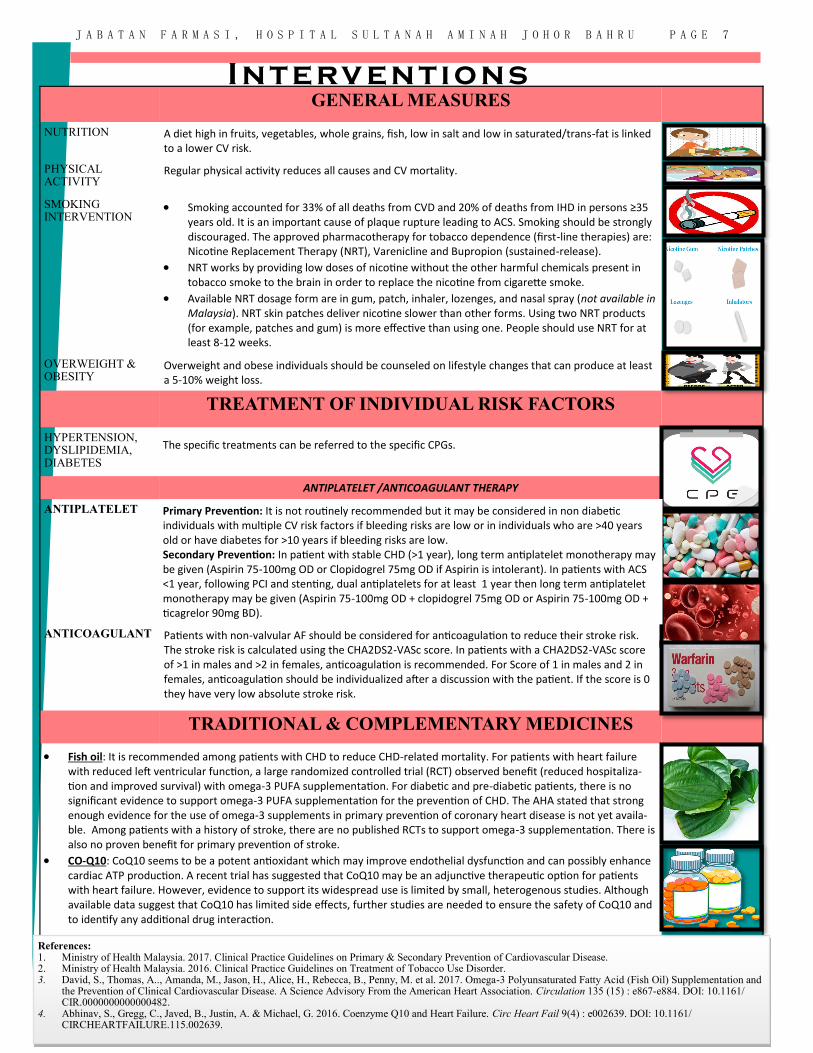
Risk Stratification of CVD Risk from
FRS Score
>30%: Very high risk
>20%: High risk
10-20%: Moderate risk
<10%: Low risk
• Most individuals who are at Low and Moderate Risk can be managed by lifestyle changes alone.
• Those at High Risk and High Lifetime Risk may require pharmacotherapy in accordance with CPGs.
Table 1A
Table 1B
PRIMARY AND SECONDARY PREVENTION OF CARDIOVASCULAR DISEASE 2017
P A G E 6 J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U
Introduction
Secondary Prevention Strategies
I nt erv entions
GENERAL MEASURES
NUTRITION A diet high in fruits, vegetables, whole grains, fish, low in salt and low in saturated/trans-fat is linked to a lower CV risk.
PHYSICAL ACTIVITY
Regular physical activity reduces all causes and CV mortality.
SMOKING INTERVENTION
• Smoking accounted for 33% of all deaths from CVD and 20% of deaths from IHD in persons ≥35 years old. It is an important cause of plaque rupture leading to ACS. Smoking should be strongly discouraged. The approved pharmacotherapy for tobacco dependence (first-line therapies) are: Nicotine Replacement Therapy (NRT), Varenicline and Bupropion (sustained-release).
• NRT works by providing low doses of nicotine without the other harmful chemicals present in tobacco smoke to the brain in order to replace the nicotine from cigarette smoke.
• Available NRT dosage form are in gum, patch, inhaler, lozenges, and nasal spray (not available in Malaysia). NRT skin patches deliver nicotine slower than other forms. Using two NRT products (for example, patches and gum) is more effective than using one. People should use NRT for at least 8-12 weeks.
OVERWEIGHT & OBESITY
Overweight and obese individuals should be counseled on lifestyle changes that can produce at least a 5-10% weight loss.
TREATMENT OF INDIVIDUAL RISK FACTORS
HYPERTENSION, DYSLIPIDEMIA, DIABETES
ANTIPLATELET /ANTICOAGULANT THERAPY
ANTIPLATELET
ANTICOAGULANT Patients with non-valvular AF should be considered for anticoagulation to reduce their stroke risk. The stroke risk is calculated using the CHA2DS2-VASc score. In patients with a CHA2DS2-VASc score of >1 in males and >2 in females, anticoagulation is recommended. For Score of 1 in males and 2 in females, anticoagulation should be individualized after a discussion with the patient. If the score is 0 they have very low absolute stroke risk.
TRADITIONAL & COMPLEMENTARY MEDICINES
• Fish oil: It is recommended among patients with CHD to reduce CHD-related mortality. For patients with heart failure with reduced left ventricular function, a large randomized controlled trial (RCT) observed benefit (reduced hospitaliza-tion and improved survival) with omega-3 PUFA supplementation. For diabetic and pre-diabetic patients, there is no significant evidence to support omega-3 PUFA supplementation for the prevention of CHD. The AHA stated that strong enough evidence for the use of omega-3 supplements in primary prevention of coronary heart disease is not yet availa-ble. Among patients with a history of stroke, there are no published RCTs to support omega-3 supplementation. There is also no proven benefit for primary prevention of stroke.
• CO-Q10: CoQ10 seems to be a potent antioxidant which may improve endothelial dysfunction and can possibly enhance cardiac ATP production. A recent trial has suggested that CoQ10 may be an adjunctive therapeutic option for patients with heart failure. However, evidence to support its widespread use is limited by small, heterogenous studies. Although available data suggest that CoQ10 has limited side effects, further studies are needed to ensure the safety of CoQ10 and to identify any additional drug interaction.
References: 1. Ministry of Health Malaysia. 2017. Clinical Practice Guidelines on Primary & Secondary Prevention of Cardiovascular Disease. 2. Ministry of Health Malaysia. 2016. Clinical Practice Guidelines on Treatment of Tobacco Use Disorder. 3. David, S., Thomas, A.., Amanda, M., Jason, H., Alice, H., Rebecca, B., Penny, M. et al. 2017. Omega-3 Polyunsaturated Fatty Acid (Fish Oil) Supplementation and
the Prevention of Clinical Cardiovascular Disease. A Science Advisory From the American Heart Association. Circulation 135 (15) : e867-e884. DOI: 10.1161/CIR.0000000000000482.
4. Abhinav, S., Gregg, C., Javed, B., Justin, A. & Michael, G. 2016. Coenzyme Q10 and Heart Failure. Circ Heart Fail 9(4) : e002639. DOI: 10.1161/CIRCHEARTFAILURE.115.002639.
The specific treatments can be referred to the specific CPGs.
Primary Prevention: It is not routinely recommended but it may be considered in non diabetic individuals with multiple CV risk factors if bleeding risks are low or in individuals who are >40 years old or have diabetes for >10 years if bleeding risks are low. Secondary Prevention: In patient with stable CHD (>1 year), long term antiplatelet monotherapy may be given (Aspirin 75-100mg OD or Clopidogrel 75mg OD if Aspirin is intolerant). In patients with ACS <1 year, following PCI and stenting, dual antiplatelets for at least 1 year then long term antiplatelet monotherapy may be given (Aspirin 75-100mg OD + clopidogrel 75mg OD or Aspirin 75-100mg OD + ticagrelor 90mg BD).
P A G E 7 J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 8
• Infertility is currently defined as 1 year of unwanted non-conception with unprotected intercourse in the fertile phase of the menstrual cycles.
• Subfertility generally describes any form of reduced fertility with prolonged time of unwanted non-conception.
• Question of subfertility must be raised after 6 cycles of unprotected inter-course without conception.
• Alcohol • Smoking • Obese women or men who have BMI >30 • Low body weight - women who have BMI< 19 and irregular menstruation
or not menstruating • Tight underwear - there is association between elevated scrotal tempera-
ture and reduced semen quality • Occupation • Recreational drug use • Frequency and timing of sexual intercourse - sexual intercourse every 2-3
days to optimise chance of pregnancy
BY JAYASANKARI D/O SEWELLENGGAM
FACTORS AFFECTING FERTILITY
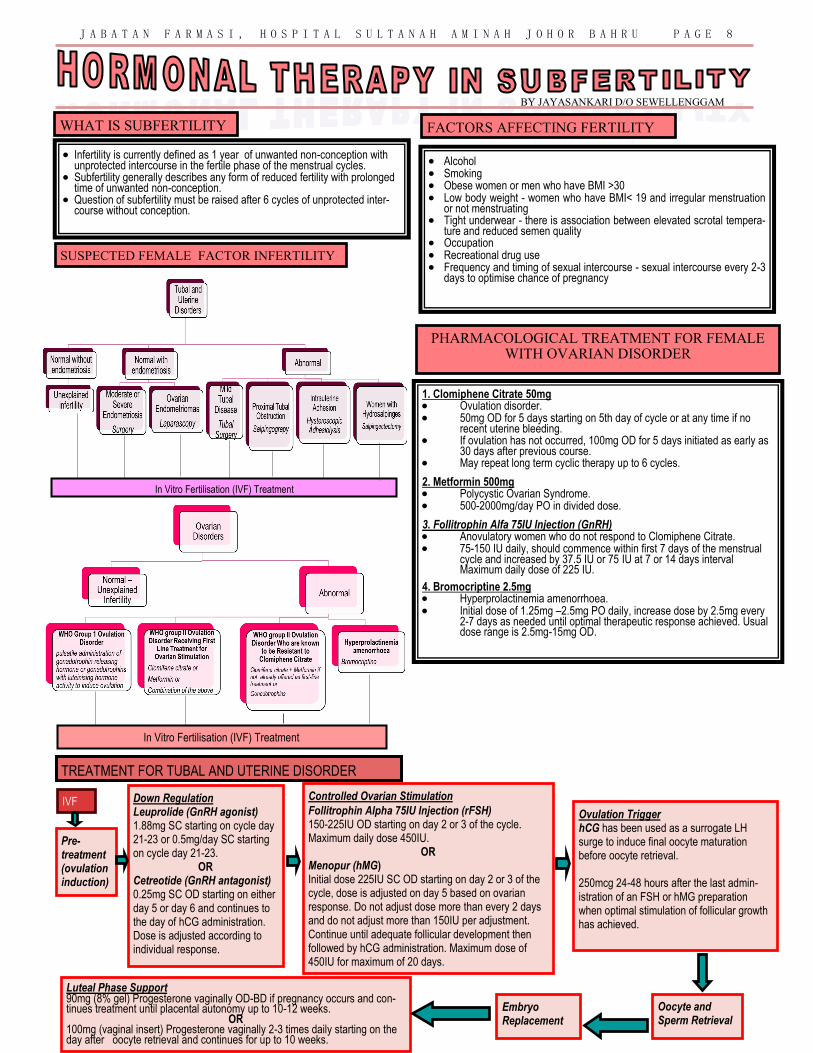
SUSPECTED FEMALE FACTOR INFERTILITY
WHAT IS SUBFERTILITY
In Vitro Fertilisation (IVF) Treatment
In Vitro Fertilisation (IVF) Treatment
PHARMACOLOGICAL TREATMENT FOR FEMALE WITH OVARIAN DISORDER
Pre-treatment (ovulation induction)
Down Regulation
Leuprolide (GnRH agonist) 1.88mg SC starting on cycle day 21-23 or 0.5mg/day SC starting on cycle day 21-23.
OR Cetreotide (GnRH antagonist) 0.25mg SC OD starting on either day 5 or day 6 and continues to the day of hCG administration. Dose is adjusted according to individual response.
Controlled Ovarian Stimulation
Follitrophin Alpha 75IU Injection (rFSH) 150-225IU OD starting on day 2 or 3 of the cycle. Maximum daily dose 450IU.
OR Menopur (hMG) Initial dose 225IU SC OD starting on day 2 or 3 of the cycle, dose is adjusted on day 5 based on ovarian response. Do not adjust dose more than every 2 days and do not adjust more than 150IU per adjustment. Continue until adequate follicular development then followed by hCG administration. Maximum dose of 450IU for maximum of 20 days.
Ovulation Trigger hCG has been used as a surrogate LH surge to induce final oocyte maturation before oocyte retrieval. 250mcg 24-48 hours after the last admin-istration of an FSH or hMG preparation when optimal stimulation of follicular growth has achieved.
Oocyte and Sperm Retrieval
Embryo Replacement
Luteal Phase Support
90mg (8% gel) Progesterone vaginally OD-BD if pregnancy occurs and con-tinues treatment until placental autonomy up to 10-12 weeks.
OR 100mg (vaginal insert) Progesterone vaginally 2-3 times daily starting on the day after oocyte retrieval and continues for up to 10 weeks.
IVF
TREATMENT FOR TUBAL AND UTERINE DISORDER
1. Clomiphene Citrate 50mg • Ovulation disorder. • 50mg OD for 5 days starting on 5th day of cycle or at any time if no
recent uterine bleeding. • If ovulation has not occurred, 100mg OD for 5 days initiated as early as
30 days after previous course. • May repeat long term cyclic therapy up to 6 cycles. 2. Metformin 500mg • Polycystic Ovarian Syndrome. • 500-2000mg/day PO in divided dose. 3. Follitrophin Alfa 75IU Injection (GnRH) • Anovulatory women who do not respond to Clomiphene Citrate. • 75-150 IU daily, should commence within first 7 days of the menstrual
cycle and increased by 37.5 IU or 75 IU at 7 or 14 days interval
Maximum daily dose of 225 IU.
4. Bromocriptine 2.5mg • Hyperprolactinemia amenorrhoea. • Initial dose of 1.25mg –2.5mg PO daily, increase dose by 2.5mg every
2-7 days as needed until optimal therapeutic response achieved. Usual dose range is 2.5mg-15mg OD.
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 9
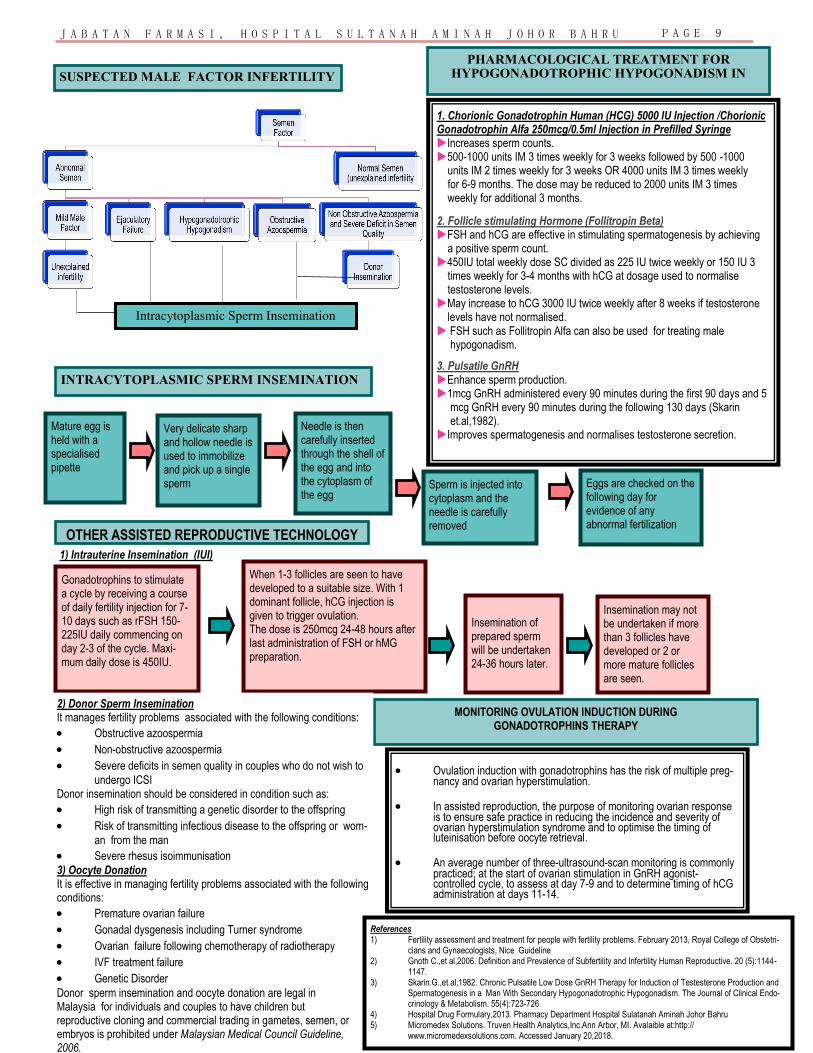
SUSPECTED MALE FACTOR INFERTILITY
Intracytoplasmic Sperm Insemination
PHARMACOLOGICAL TREATMENT FOR HYPOGONADOTROPHIC HYPOGONADISM IN
1. Chorionic Gonadotrophin Human (HCG) 5000 IU Injection /Chorionic Gonadotrophin Alfa 250mcg/0.5ml Injection in Prefilled Syringe Increases sperm counts. 500-1000 units IM 3 times weekly for 3 weeks followed by 500 -1000 units IM 2 times weekly for 3 weeks OR 4000 units IM 3 times weekly for 6-9 months. The dose may be reduced to 2000 units IM 3 times weekly for additional 3 months.
2. Follicle stimulating Hormone (Follitropin Beta) FSH and hCG are effective in stimulating spermatogenesis by achieving a positive sperm count. 450IU total weekly dose SC divided as 225 IU twice weekly or 150 IU 3 times weekly for 3-4 months with hCG at dosage used to normalise testosterone levels. May increase to hCG 3000 IU twice weekly after 8 weeks if testosterone levels have not normalised. FSH such as Follitropin Alfa can also be used for treating male hypogonadism. 3. Pulsatile GnRH Enhance sperm production. 1mcg GnRH administered every 90 minutes during the first 90 days and 5 mcg GnRH every 90 minutes during the following 130 days (Skarin et.al,1982). Improves spermatogenesis and normalises testosterone secretion.
INTRACYTOPLASMIC SPERM INSEMINATION
Mature egg is held with a specialised pipette
Very delicate sharp and hollow needle is used to immobilize and pick up a single sperm
Needle is then carefully inserted through the shell of the egg and into the cytoplasm of the egg
Sperm is injected into cytoplasm and the needle is carefully removed
Eggs are checked on the following day for evidence of any abnormal fertilization
1) Intrauterine Insemination (IUI)
MONITORING OVULATION INDUCTION DURING GONADOTROPHINS THERAPY
• Ovulation induction with gonadotrophins has the risk of multiple preg-nancy and ovarian hyperstimulation.
• In assisted reproduction, the purpose of monitoring ovarian response is to ensure safe practice in reducing the incidence and severity of ovarian hyperstimulation syndrome and to optimise the timing of luteinisation before oocyte retrieval.
• An average number of three-ultrasound-scan monitoring is commonly practiced; at the start of ovarian stimulation in GnRH agonist-controlled cycle, to assess at day 7-9 and to determine timing of hCG administration at days 11-14.
Gonadotrophins to stimulate a cycle by receiving a course of daily fertility injection for 7-10 days such as rFSH 150-225IU daily commencing on day 2-3 of the cycle. Maxi-mum daily dose is 450IU.
When 1-3 follicles are seen to have developed to a suitable size. With 1 dominant follicle, hCG injection is given to trigger ovulation. The dose is 250mcg 24-48 hours after last administration of FSH or hMG preparation.
Insemination of prepared sperm will be undertaken 24-36 hours later.
Insemination may not be undertaken if more than 3 follicles have developed or 2 or more mature follicles are seen.
OTHER ASSISTED REPRODUCTIVE TECHNOLOGY
2) Donor Sperm Insemination It manages fertility problems associated with the following conditions:
• Obstructive azoospermia
• Non-obstructive azoospermia
• Severe deficits in semen quality in couples who do not wish to
undergo ICSI Donor insemination should be considered in condition such as:
• High risk of transmitting a genetic disorder to the offspring
• Risk of transmitting infectious disease to the offspring or wom-
an from the man
• Severe rhesus isoimmunisation
3) Oocyte Donation It is effective in managing fertility problems associated with the following conditions:
• Premature ovarian failure
• Gonadal dysgenesis including Turner syndrome
• Ovarian failure following chemotherapy of radiotherapy
• IVF treatment failure
• Genetic Disorder
Donor sperm insemination and oocyte donation are legal in Malaysia for individuals and couples to have children but reproductive cloning and commercial trading in gametes, semen, or embryos is prohibited under Malaysian Medical Council Guideline, 2006.
References 1) Fertility assessment and treatment for people with fertility problems. February 2013, Royal College of Obstetri-
cians and Gynaecologists, Nice Guideline 2) Gnoth C.,et al,2006. Definition and Prevalence of Subfertility and Infertility Human Reproductive. 20 (5):1144-
1147. 3) Skarin.G.,et.al,1982. Chronic Pulsatile Low Dose GnRH Therapy for Induction of Testesterone Production and
Spermatogenesis in a Man With Secondary Hypogonadotrophic Hypogonadism. The Journal of Clinical Endo-crinology & Metabolism. 55(4):723-726
4) Hospital Drug Formulary,2013. Pharmacy Department Hospital Sulatanah Aminah Johor Bahru 5) Micromedex Solutions. Truven Health Analytics,Inc.Ann Arbor, MI. Avalaible at:http://
www.micromedexsolutions.com. Accessed January 20,2018.

LAPORAN AKTIVITI BERGAMBAR PAMERAN KUA
BERSEMPENA HARI BUAH PINGGANG SEDUNIA 2018 Oleh Lee Chui Peng
Pameran KUA telah diadakan sempena Hari Buah Pinggang Sedunia 2018
yang bertajuk ‘Buah Pinggang dan Kesihatan Wanita’ pada 11 March 2018 di
JBCC Komtar Johor Bahru. Program Hari Buah Pinggang Sedunia dianjurkan oleh
National Kidney Foundation dan dirasmikan oleh YB Datuk Haji Ayub Bin Rahman.
Tujuan pameran adalah untuk meningkatkan kesedaran dan pengetahuan
mengenai penggunaan ubat secara rasional di kalangan orang awam. Sudut
kaunseling juga disediakan untuk memberi kaunseling kepada orang awam
mengenai ubat-ubatan.
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 1 0