lumbar canal stenosis
TRANSCRIPT
MEDANTA BONE & JOINT INSTITUTE
MODERATORS: DR. VINEESH MATHURDR DHARMENDER SINGH
PRESENTED BY:DR HIMANSHU BANSAL
DefinitionSTENOSIS Constriction of a tube.
Spinal canal stenosis is defined as an abnormal narrowing of OSTEOLIGAMENTOUS vertebral canal and/or the Intervertebral foramina, causing direct compression or compromise of the dural sac/ caudal nerve root or their vasculature.
producing symptom of radiculopathy or claudication.
History • 1803 Portal {French anatomist}, first reported
cord compression and paralysis in children severely deformed by rickets
• 1891 Gowers considered the possibility of lateral stenosis. He noted that narrowing of the foramina may damage the nerve roots and radiating pains may be produced.
• 1910 Sumita described narrow vertebral Canal in Achondroplastic Dwarfs.
• 1920 Putti wrote about nerve root entrapment caused by degenerative changes in the facet joints.
• Verbiest had a major contribution• In 1949 he described narrow vertebral canal in
patients without any disease or pathological condition in the classic sense.
• The narrowness was due to an isolated growth disturbance of the vertebral arch.
• He coined the term "developmental stenosis". • In 1954 he redescribed this clinical syndrome
with his operative studies, showing bony changes producing narrowed spinal canal particularly in the sagittal plane.
History
CLINICAL ANATOMY
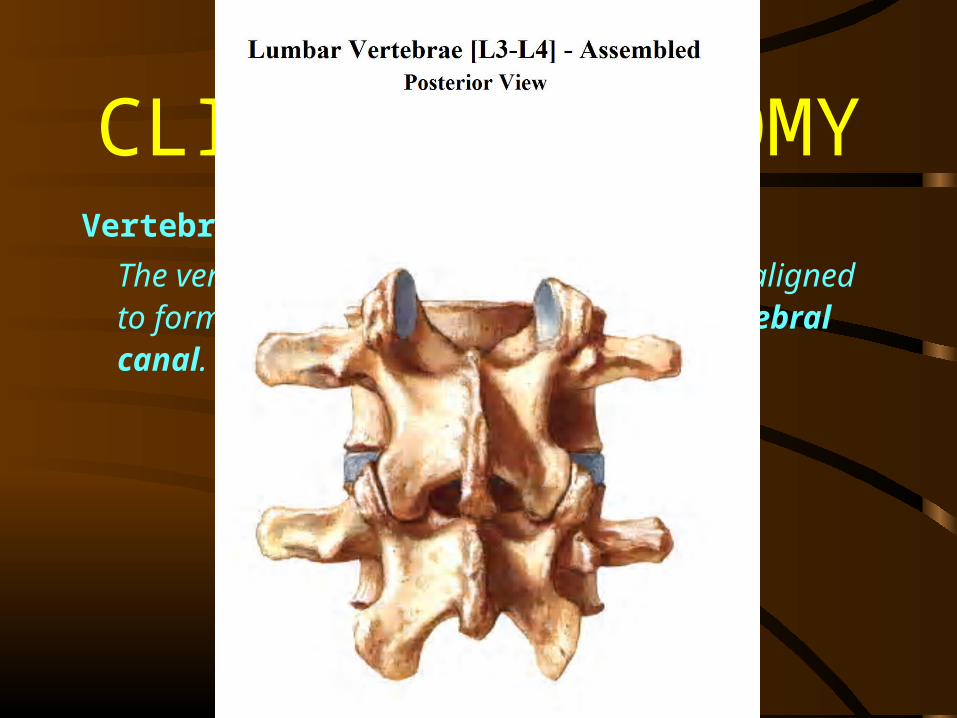
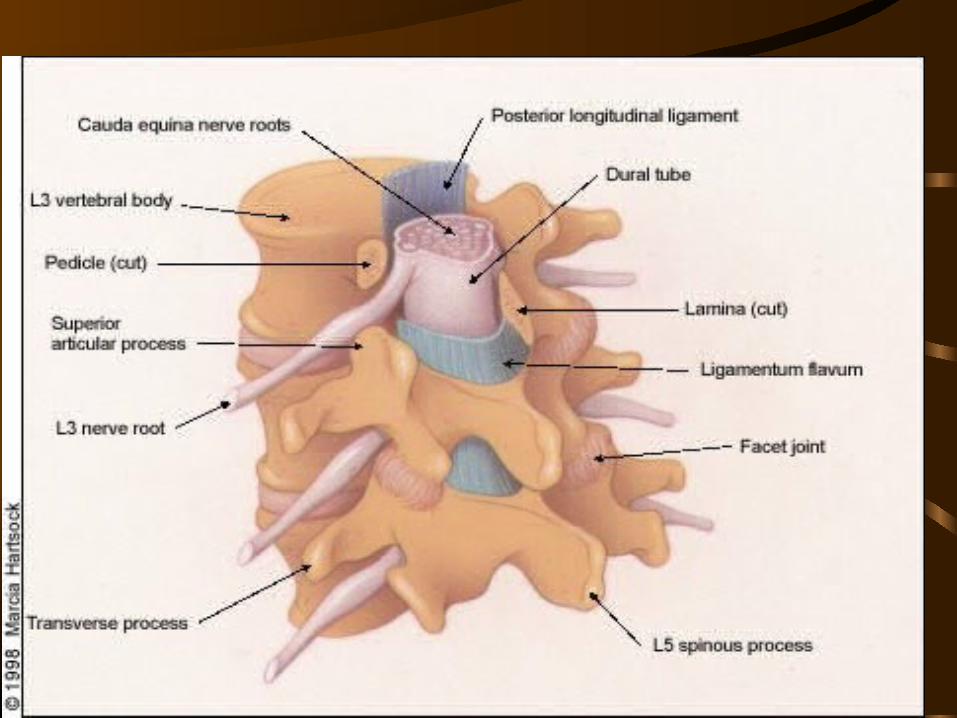
Vertebral CanalThe vertebral foramina of the vertebrae are aligned to form a continuous channel called the Vertebral canal.
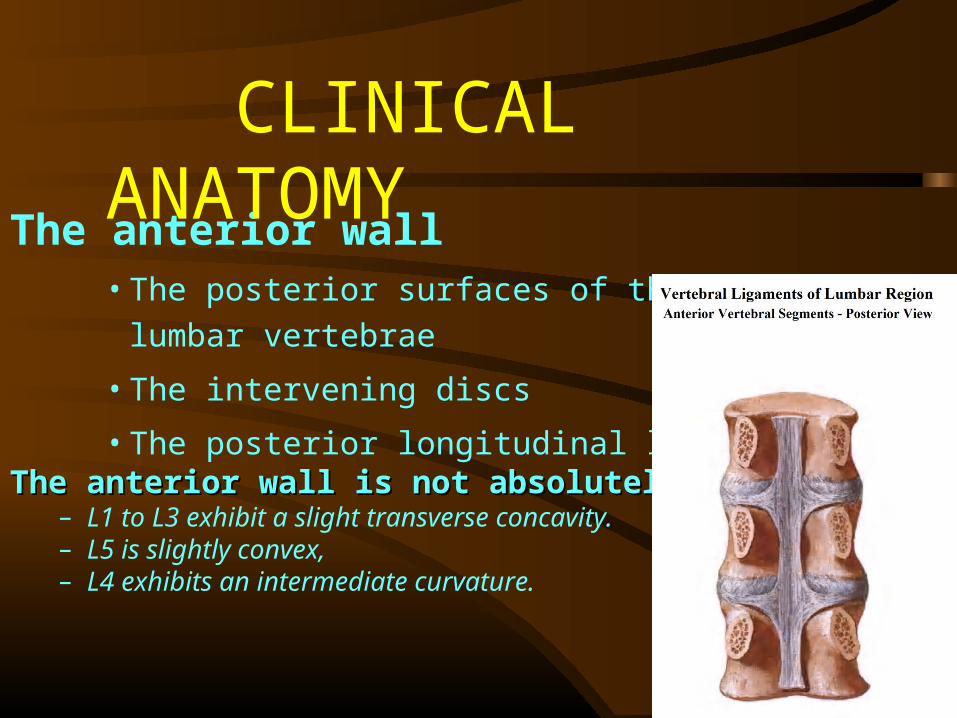
The anterior wall• The posterior surfaces of the lumbar vertebrae
• The intervening discs
• The posterior longitudinal ligamentThe anterior wall is not abso lutely flatThe anterior wall is not abso lutely flat.
– L1 to L3 exhibit a slight transverse concavity. – L5 is slightly convex, – L4 exhibits an intermediate curvature.
CLINICAL ANATOMY
• The posterior wall- The laminae of the vertebrae and the intervening ligamenta flava.
• The lateral wall -The pedicles of the lumbar vertebrae. Between the pedicles, the lateral wall is deficient where the superior and inferior vertebral notches appose one another to form the intervertebral foramina.
CLINICAL ANATOMY
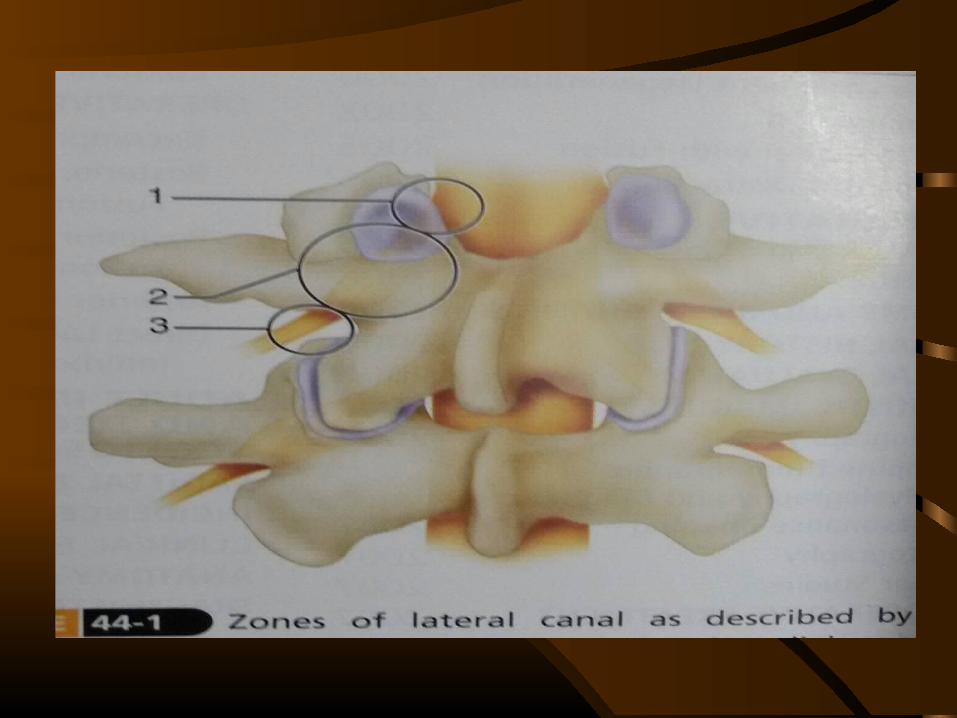
Lee et al classified based on type of surgical decompression indicated
• The retrodiscal segment{ENTRANCE ZONE}
• The parapedicular segment {MID ZONE}
• The third segment { EXIT ZONE}
LATERAL CANAL
The Retrodiscal Segment, { ENTRANCE ZONE}
Anterior wall - By the intervertebral disc in this region,
Posterior wall- by the facet joint.Lateral wall- pediclesMedial wall- central canal
Stenosis - By facet arthritis, vertebral body spurring and disc or annulus pathology.
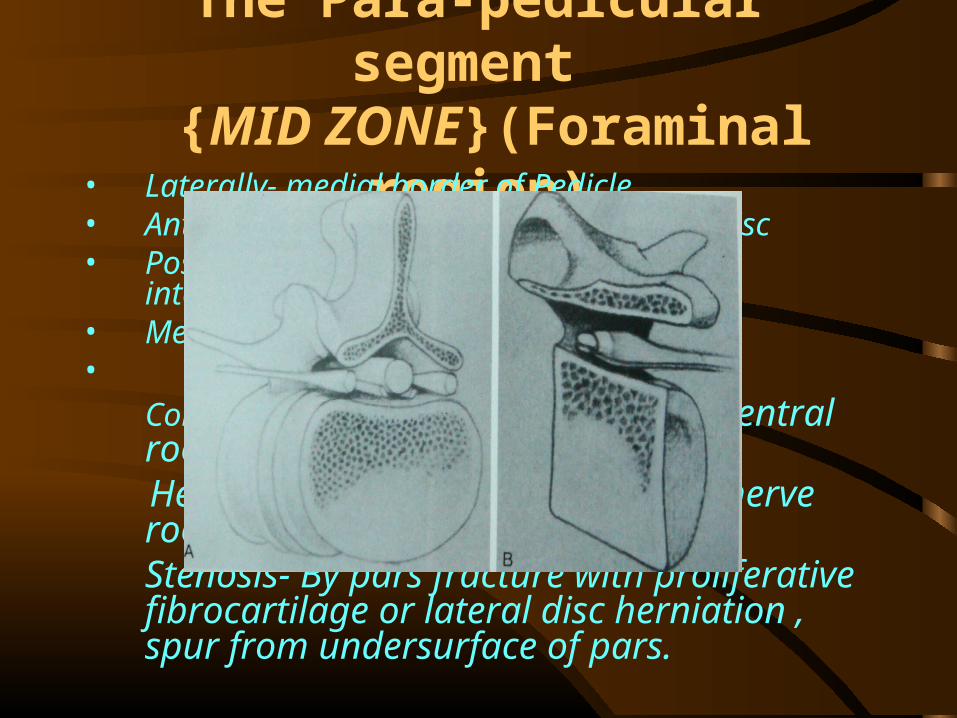
The Para-pedicular segment {MID ZONE}(Foraminal region)
• Laterally- medial border of Pedicle• Anteriorly- Posterior vertebral body and disc• Posteriorly- Pars interarticularis and
intertransverse ligament• Medially – Lateral recess•
Contents - Dorsal root ganglion and ventral root. Here dura becomes confluent with nerve root as
epineurium.Stenosis- By pars fracture with proliferative fibrocartilage or lateral disc herniation , spur from undersurface of pars.
The third segment { EXIT ZONE}
• It’s an area lateral to the facet joint.• It contains nerve roots.
Stenosis - By ‘far lateral ’ disc,spondylolisthesis, hypertrophic facets with subluxation.
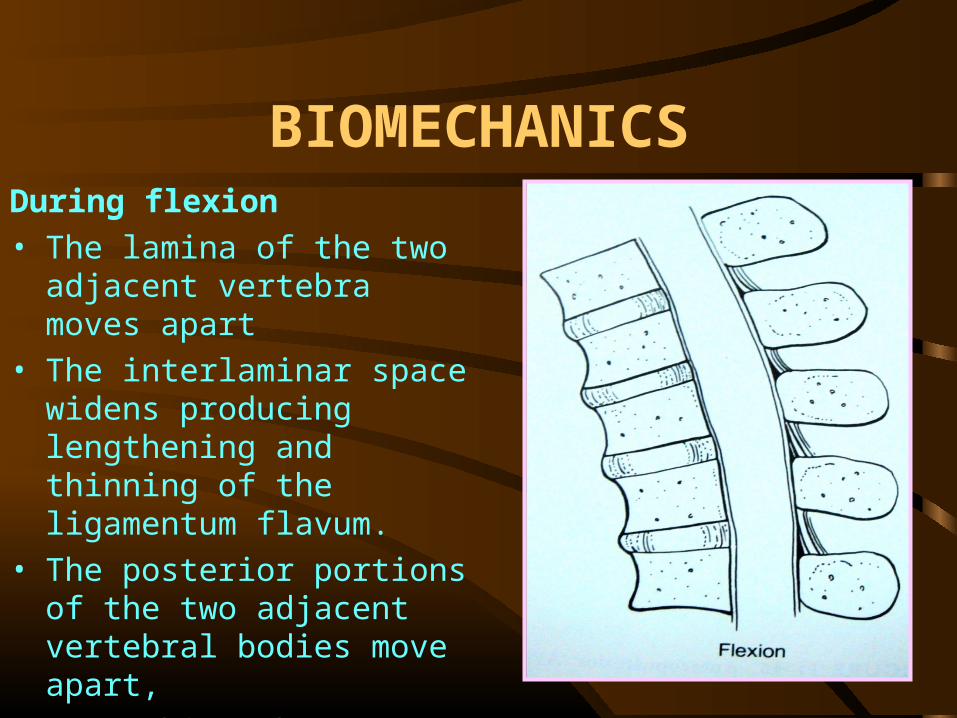
BIOMECHANICSDuring flexion • The lamina of the two adjacent
vertebra moves apart • The interlaminar space widens
producing lengthening and thinning of the ligamentum flavum.
• The posterior portions of the two adjacent vertebral bodies move apart,
• Stretching the posterior portion of annulus fibrosus.
BIOMECHANICS
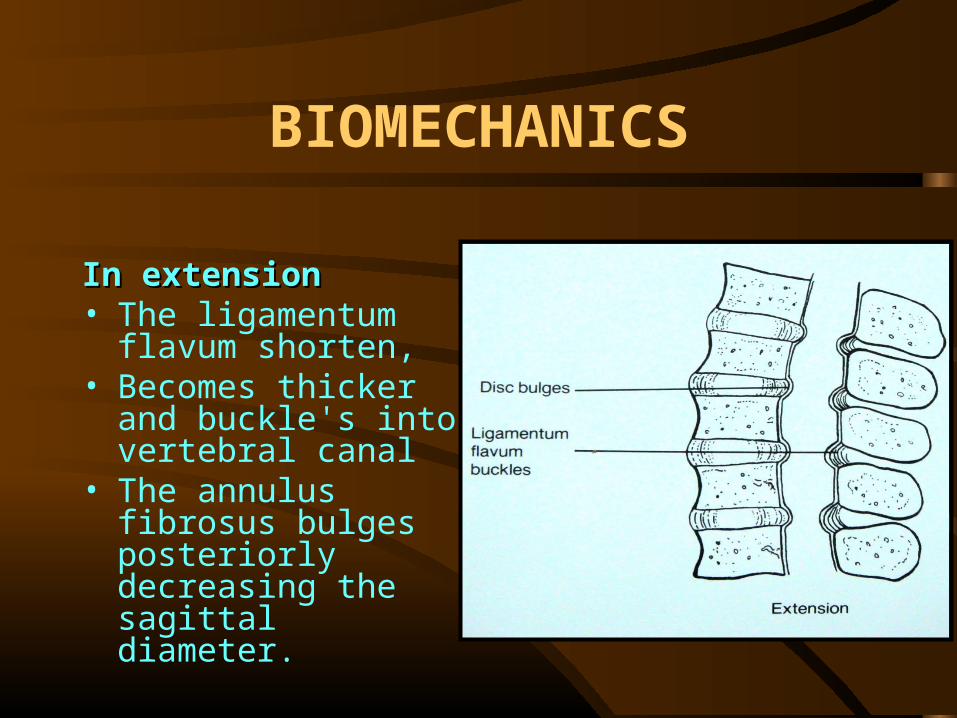
In extensionIn extension • The ligamentum flavum
shorten, • Becomes thicker and
buckle's into vertebral canal
• The annulus fibrosus bulges posteriorly decreasing the sagittal diameter.
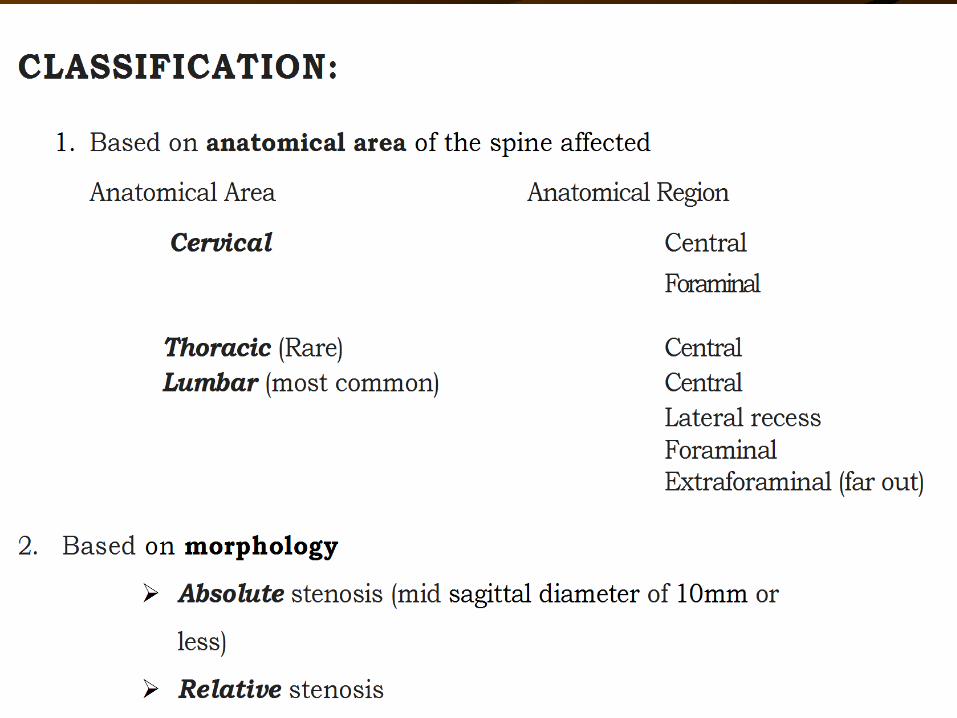

PATHOANATOMY• The Stenosing pathology could be either of
Narrowing or Encroaching nature. • The Narrowing pathology are developmental
• Encroaching pathology are Degenerative• The encroaching pathologies could be
• Static • Dynamic

Anteriorly
Posteriorly
Posterolateral
Static encroachmentUpper and lower marginal osteophytes from body Calcified annulus with or without nucleusInturned proximal margin of laminaOsteophytes at the laminar attachment of lig. FlavumThickened and enlarged superior articular process Low lying ligamentum flavum forming roof of root canal. Thickened and hypertrophied anteromedial capsule of the facet joint.
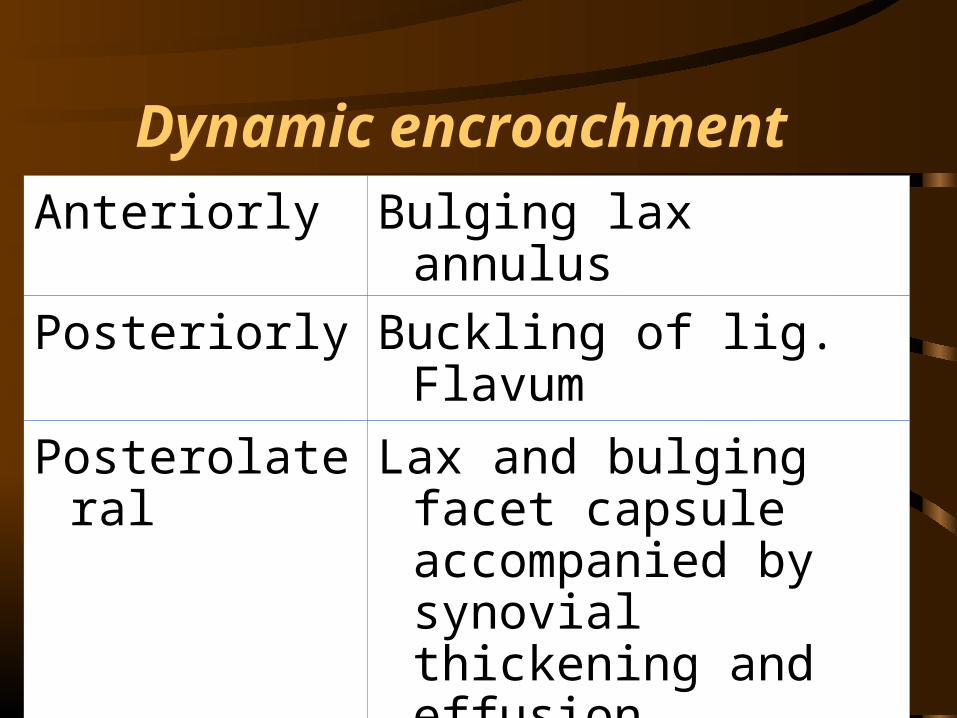
Anteriorly Bulging lax annulusPosteriorly Buckling of lig.
FlavumPosterolatera
lLax and bulging facet
capsule accompanied by synovial thickening and effusion
Dynamic encroachment
The type-I collagen content increases in the discs of individuals who are middle-aged & The type-I collagen content increases in the discs of individuals who are middle-aged & older. With age and subsequent degeneration, the total proteoglycan content decreases. older. With age and subsequent degeneration, the total proteoglycan content decreases.
The rate of proteoglycan synthesis also decreases with age.The rate of proteoglycan synthesis also decreases with age.
The biomechanical & biochemical changes lead to decrease in disc height, annular The biomechanical & biochemical changes lead to decrease in disc height, annular bulging, disc herniation, & early osteophyte formation.bulging, disc herniation, & early osteophyte formation.
Increased biomechanical stresses are transmitted posteriorly to the facet joints. Increased biomechanical stresses are transmitted posteriorly to the facet joints. arthritic changes and occasionally, facet hypertrophy, instability of the facet joints may arthritic changes and occasionally, facet hypertrophy, instability of the facet joints may
developdevelop As the disc degenerates & the cephalocaudal foraminal space narrows, nerve root As the disc degenerates & the cephalocaudal foraminal space narrows, nerve root entrapment can occur, resulting in stenosis both centrally & in the lateral recess. entrapment can occur, resulting in stenosis both centrally & in the lateral recess.
With age, the water content decreases. As the nucleus pulposus With age, the water content decreases. As the nucleus pulposus dehydrates, its ability to distribute stress diminishes, leading to fissures & dehydrates, its ability to distribute stress diminishes, leading to fissures &
tears within the annulustears within the annulus
DEGENERATIVE STENOSIS
Pathophysiology ofClaudication Pain
A decrease in blood flow The blood supply to the cauda equina and the
spinal nerve roots is from cephalad to caudad along the cauda equina
And from caudad to cephalad as it traverses the neuroforamen across the dorsal root ganglia.
Compression in any of these locations can interfere with the vascular supply and nutritional support to the nerve roots, the cauda equina, or the dorsal root ganglia or any combination of these structures.
The stenotic spinal canal compresses the dural sac or nerve root and its vasculature.
The pathophysioiogy of neurogenic claudication can be explained in terms of pathologic condition at multiple levels i.e.
Central stenosis at a single level or an isolated root canal stenosis does not account for this symptom.
Either a two level central stenosis or a central stenosis associated with root canal stenosis must be present for neurogenic claudication.
VENOUS CONGESTION
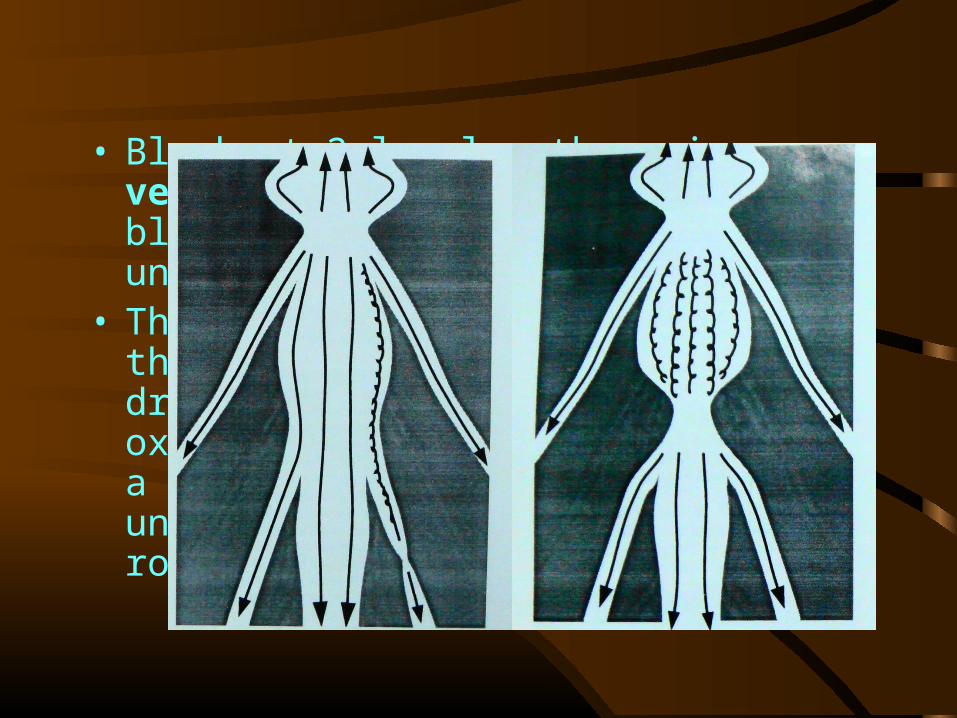
• Block at 2 levels -there is venous congestion and pooling of blood between the 2 blocks at the uncompressed segment.
• The arterioles continue to feed the segment, but impaired drainage reduces the blood flow, oxygen supply and nutrition, with a build up of metabolites in the uncompressed segment of the nerve root or cauda equina.
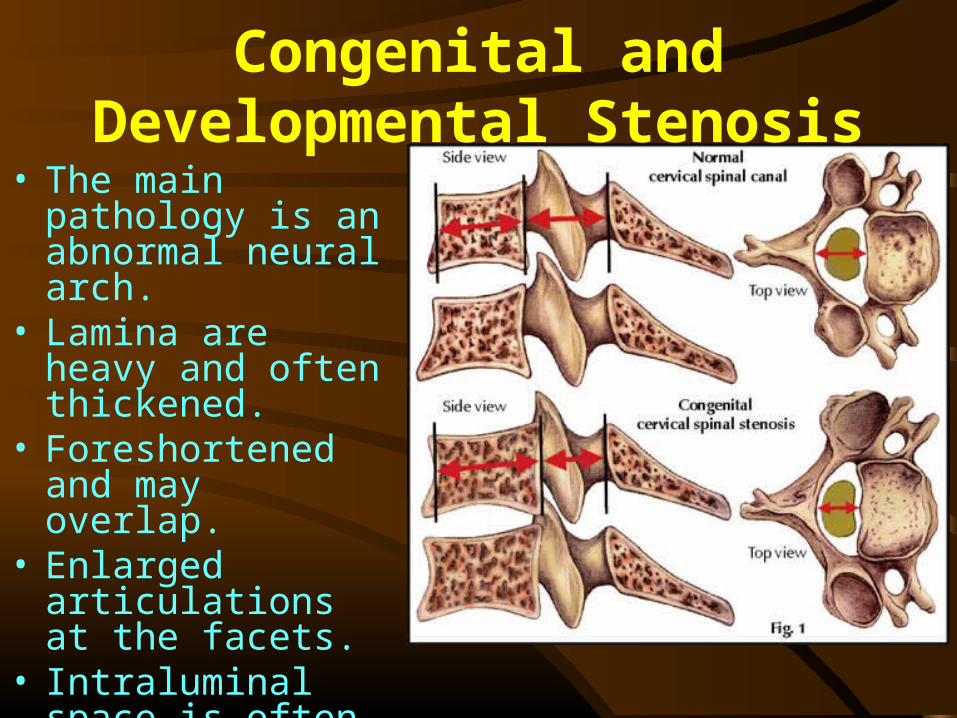
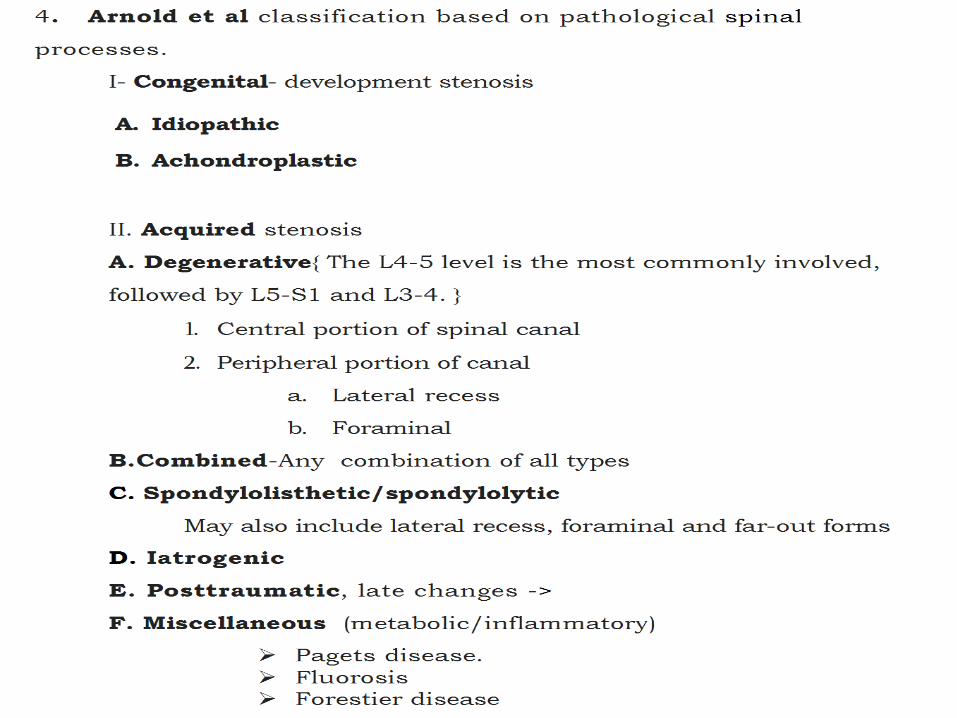
Congenital and Developmental Stenosis
• The main pathology is an abnormal neural arch.
• Lamina are heavy and often thickened.
• Foreshortened and may overlap.
• Enlarged articulations at the facets.
• Intraluminal space is often oblitered.
• There is an uniform narrowing of the whole of the lumbar spinal canal more marked in the AP than in the transverse diameter
Congenital and Developmental Stenosis
• Iatrogenic: Complication of spinal surgery (post laminectomy or post fusion),post chemonucleolysis
• Post-traumatic: Following a burst fracture of a vertebral body.
Further narrowing of the canal may result from degenerative changes with new bone formation over a period of years.
• Metabolic: • Flurosis:
» Changes seen here resemble degenerative stenosis.
» There is florid new bone formation, irregular in contour.
• Paget's disease: » Whole vertebral body becomes
enlarged and the posterior aspect comes to protrude posteriorly and narrows the spinal canal.
Clinical Features• Most commonly in males over 40 years. • Natural course is Insidious development of
symptoms occasionally exacerbated by trauma or heavy activity.
• Back pain in 95%• Sciatica in 91%. • Sensory disturbance in the legs in 70% • Motor weakness in 33%,• Voiding disturbance present in only 12%.
• The classic symptom pattern of stenosis is that of neurogenic claudication.
Clinical Features
Neurogenic Claudication• Verbiest defined neurogenic intermittent claudication
as the onset of pain, tension and weakness upon walking in one or both legs progressively increasing until walking becomes impossible and subsequent disappearance of symptoms after a period of rest(20 minutes).
• Should not be present before walking but should occur during walking.
• Disappear after a short rest by sitting and bending forward or crouching.
• Pain increases with standing and walking. • The patient may obtain the ‘Simian stance'
to obtain relief. • Hypoasthesia, paraesthesia are often
precipitated by exercise. • Walking uphill or riding a bicycle may be
done with ease but walking down hill produces pain.
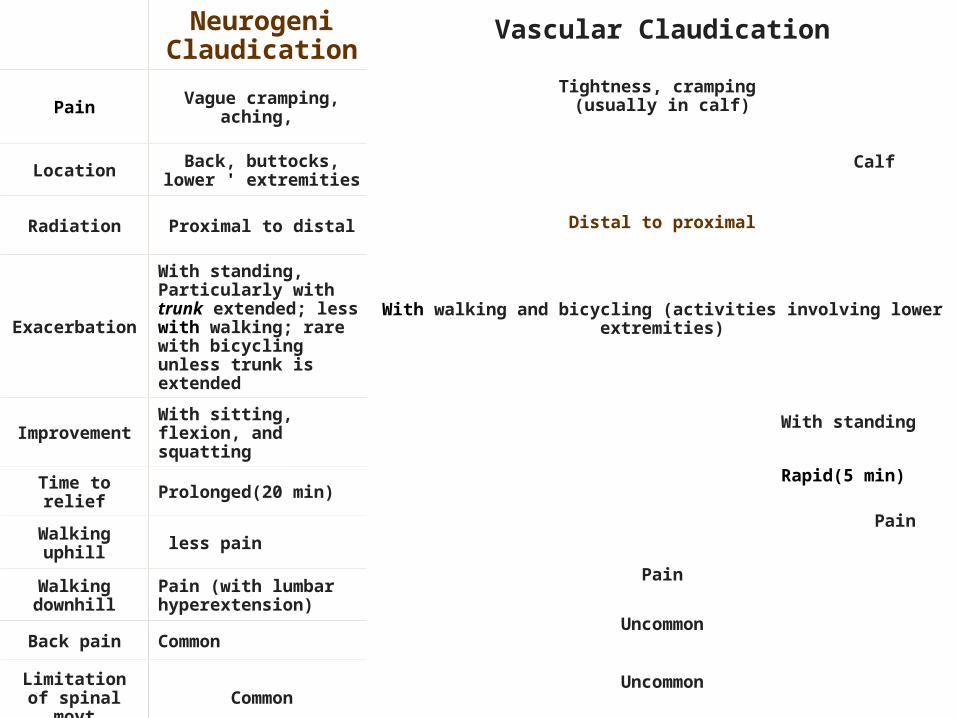
Neurogeni Claudication
Pain Vague cramping, aching,
Location Back, buttocks, lower ' extremities
Radiation Proximal to distal
Exacerbation
With standing, Particularly with trunk extended; less with walking; rare with bicycling unless trunk is extended
Improvement
With sitting, flexion, and squatting
Time to relief Prolonged(20 min)
Walking uphill less pain
Walking downhill
Pain (with lumbar hyperextension)
Back pain Common
Limitation of spinal movt Common
Vascular Claudication
Tightness, cramping (usually in calf)
Calf
Distal to proximal
With walking and bicycling (activities involving lower extremities)
With standing
Rapid(5 min)
Pain
Pain
Uncommon
Uncommon
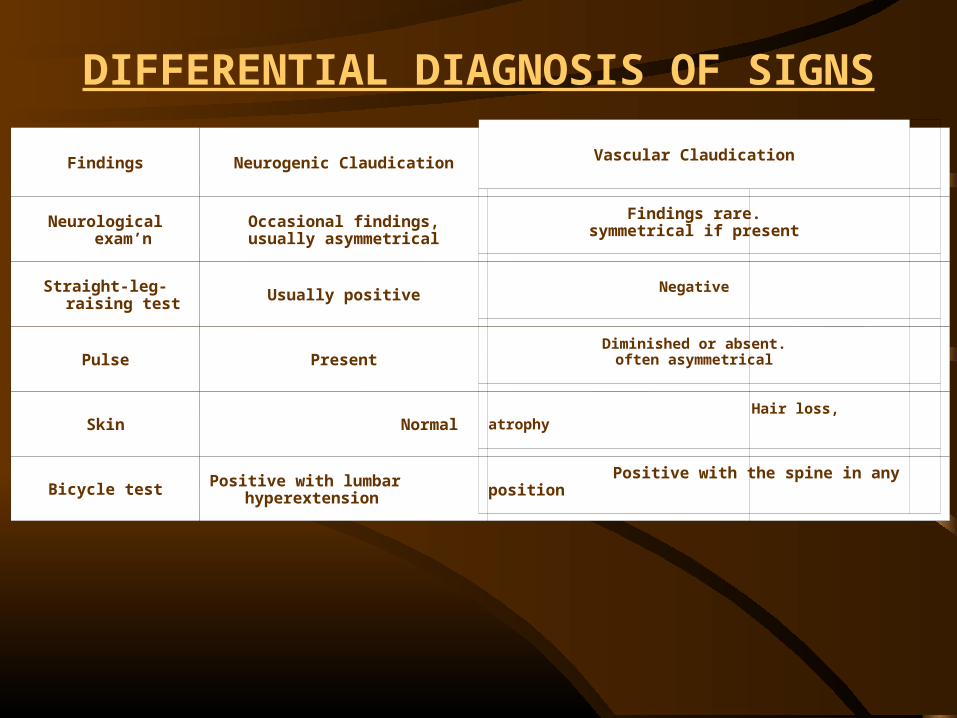
Findings Neurogenic Claudication
Neurological exam’n
Occasional findings,usually asymmetrical
Straight-leg-raising test Usually positive
Pulse Present
Skin Normal
Bicycle test Positive with lumbar hyperextension
Vascular Claudication
Findings rare.symmetrical if present
Negative
Diminished or absent.often asymmetrical
Hair loss, atrophy
Positive with the spine in any position
DIFFERENTIAL DIAGNOSIS OF SIGNS

Physical Findings• Minimal and nonspecific at rest, • Most common - Decreased lumbosacral
motion. • Neurological findings -muscle weakness
and areas of sensory loss. • They may be detected more rapidly if the
patient is examined shortly after performing exercise.
• Straight leg raising test is usually normal but may be present.
STOOP TEST
• This test is done by asking the patient to walk briskly.
• As the pain intensifies, the patient may complain of sensory symptoms followed by motor symptoms.
• If the patient is asked to continue to walk, he may assume a stooped posture, and the symptoms may be eased;
• If he sits in a chair bent forward, the same resolution of symptoms will occur.
• Distal pulses should be felt and confirmed to be strong,
• Internal and external rotation of the hips in extension should be full, symmetrical, and painless.
Investigations:
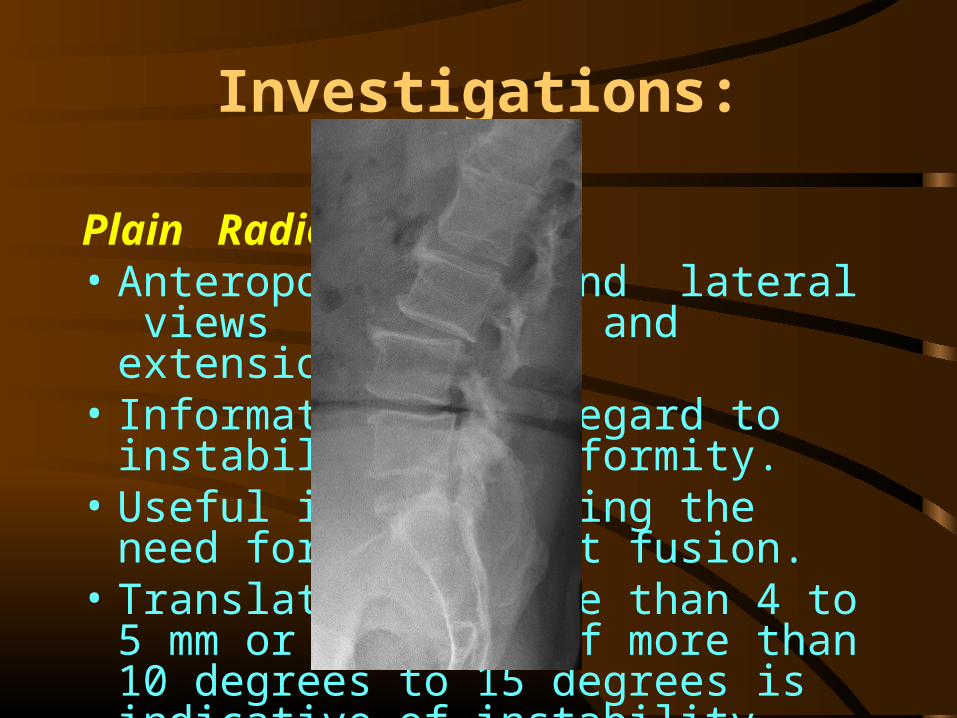
Plain Radiographs:• Anteroposterior and lateral views in
flexion and extension • Information with regard to instability and
deformity. • Useful in determining the need for
subsequent fusion.• Translation of more than 4 to 5 mm or
rotation of more than 10 degrees to 15 degrees is indicative of instability.
MRI Scan
• It is an excellent diagnostic tool • It provides information about both the
bony and soft tissue structures. • It has rapidly become the imaging
study of choice for the diagnosis of spinal stenosis
MRI Scan
Advantages:• It gives useful information about the size
and contour of the foramen and conus and helps to assess the extradural CSF interface and central canal dimensions.
• There is no radiation exposure and it is non-invasive
• Entire lumbar spine is imaged
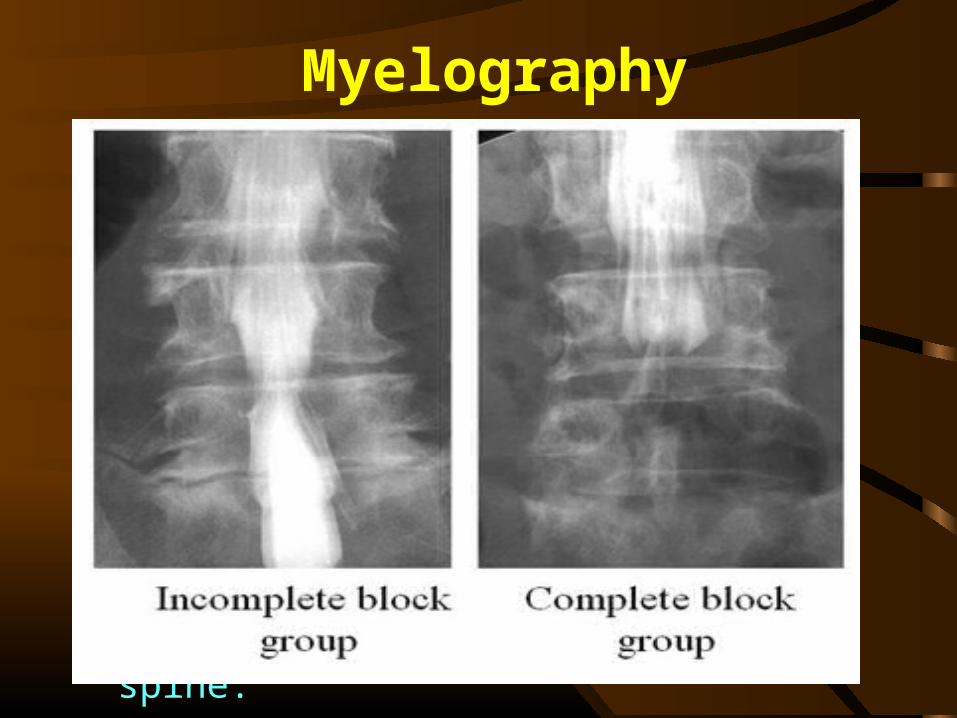
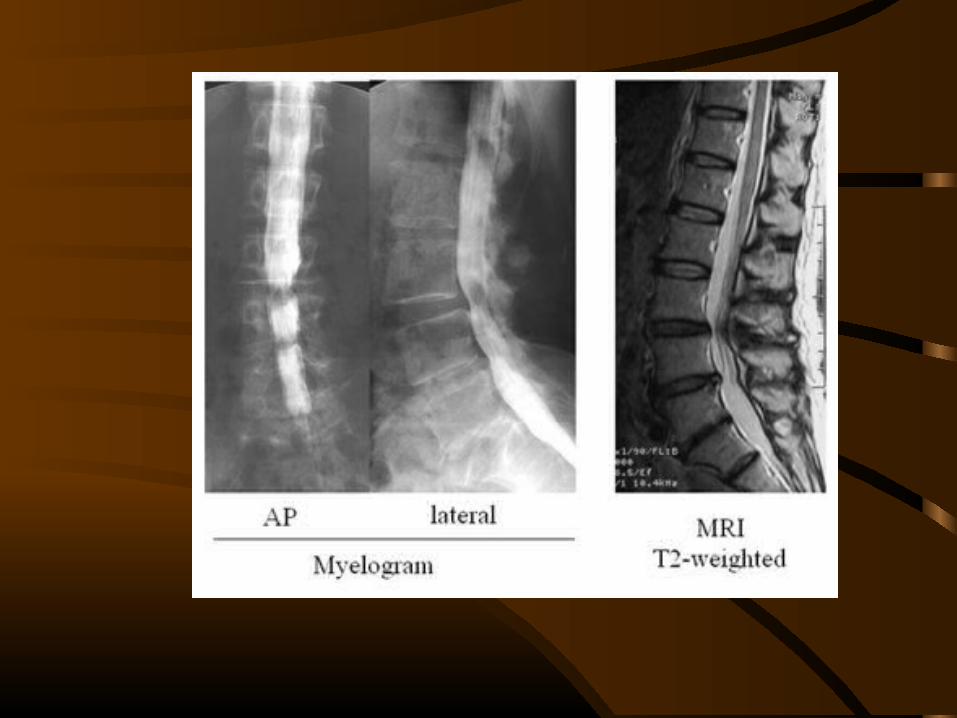
Myelography
Advantages:• The entire lumbar spine is visualized • Lesions of the conus may be detected. • Unsuspected levels of stenosis proximal to L3
may also be detected.• It can be a dynamic imaging tool i.e. spinal canal
can be examined with the flexed and hyperextended spine.
• Samples of CSF can be obtained.
C T Scan
Advantages:• It allows direct visualization of the offending
agents such as osteophytes, (enlarged facets etc). • It can be combined with myelogram for obtaining
more details. • A mid sagittal diameter of 10mm or less and AP
diameter of the lateral recess of 3 mm or less is considered abnormal.
C T Scan
Advantages:• Sagittal reconstructions are useful in assessing
foraminal stenosis. • Loss of epidural fat can be fairly well delineated. • Often in elderly patients with pacemaker or other
metal implants contraindicating MRI, a CT myelogram is the only reliable imaging study before surgery
Electro Diagnostic StudiesElectromyography • Evaluates physiology
of nerve roots, which is useful in delineating diseases of the lower, motor neuron units.
• It is abnormal in about 80% of patients with spinal stenosis and provides confirmatory evidence of level of nerve root involvement.
Electro Diagnostic StudiesNerve conduction studies: • It measures the speed at which the nerve impulse travels. • It is most useful in differentiating peripheral
neuropathy from radiculopathy.
Somatosensory evoked potentials. • These studies are often useful and more sensitive than
EMGs in identifying the level of nerve root compression thus indicating the level of symptomatic stenosis.
• It also has a high rate of false positive readings. • Should always be read in conjunction with the imaging
studies.
Treatment
The treatment strategy depends on• The severity of clinical symptom• Type of stenosis• Extent of stenosis• Any associated instability or deformity
Non-operative treatment {Conservative}
• Give the option of nonoperative treatment. • If the patient fails to improve after a trial of
conservative care, he or she can expect to have a good result from surgery.
• No predictor of successful outcome after surgical or conservative treatment.
• Delayed surgical intervention does not deny the benefit of the operation.
Non-operative treatment {Conservative}
• Activity modification is the mainstay of non-surgical treatment.
• Conservative measures should include, rest not exceeding 2 days, pain management with antiinflammatory medications or acetaminophen, and participation in a trunk-stabilization exercise program, along with good aerobic fitness.
• Traction has no proven benefit in the adult lumbar spine.
• A short period of relative rest recommended for the flare ups of symptoms
• This should be followed by exercises, particularly the flexion exercises, stationary bicycle riding partially flexed forward, aquatic exercises, and partially unloaded treadmill exercises are helpful.
Non-operative treatment {Conservative}
Non-operative treatment {Conservative}
• Pain medications - with associated risks of gastro intestinal ulceration and renal impairment in the elderly population.
• Antidepressants in low doses are occasionally helpful as an adjuvant to the pain medication, particularly in controlling neuropathic pain.
• Calcitonin treatment in lumbar spinal stenosis has been established to be beneficial in pagets disease.
Non-operative treatment {Conservative}
• Epidural steroid injections are used more frequently yet remain controversial.
• The ideal candidate for epidural steroid injection appears to be a patient who has acute radicular symptoms or neurogenic claudication unresponsive to traditional analgesics and rest, with significant impairment in activities of daily living.
Surgical Treatment
• The Goals of Surgery are • pain relief, • increased mobility and • prevention of neurological deficit.
Indications for surgery
• Increasing pain resistant to conservative treatment .
• Presence of neurological deficits. • Patients’s inability to tolerate the restricted
lifestyle
• A complete decompression of the all the involved neural elements is the key
• Preservation of spinal stability is critical • The keys to avoid iatrogenic instability are
preservation of facet joint integrity and protection of the pars.
• When adequate decompression obligates excision of facets or pars, fusion may need to be added.
Surgical Treatment
Principles of spinal stenosis surgery
Decompression by Laminectomy- In older patients with severe and multilevel stenosis
Fenestration procedures(Bilateral laminotomy or partial facetectomy)- In younger patients with intact disc
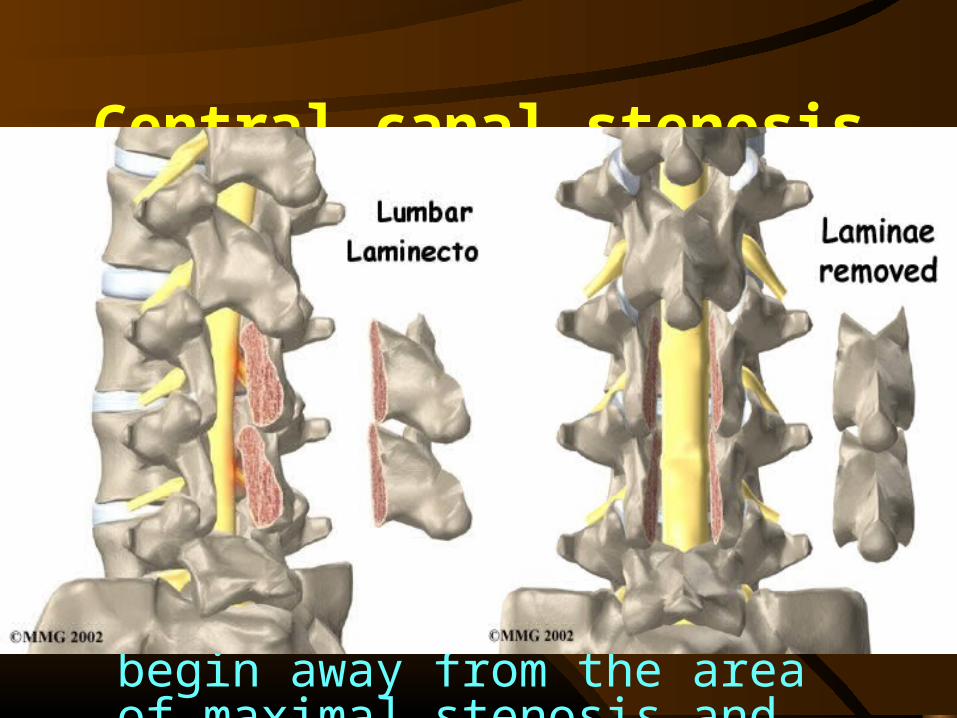
Central canal stenosis
• Central canal stenosis is treated by lumbar laminectomy at the stenotic segment.
• The spinous process and the lamina are exposed out to, but not including, the facet joints.
• The decompression should begin away from the area of maximal stenosis and should be carried out from caudal to cephalad direction.
Lateral canal stenosis
• When the stenosis is confined to the lateral recess, the nerve root may be decompressed by unilateral laminotomy.
• The spine is approached by midline incision, but only the symptomatic side is exposed.
Fusion can be done in conjunction with decompression in …
• Patients younger than 60 years of age with instability caused by the loss of an articular process on one side
• Patients younger than 55 years of age with a midline decompression for degenerative spondylolisthesis that preserves the facets
• Patients younger than 50 years of age with isthmic spondylolisthesis.
• Recurrent stenosis at the same or adjacent level previous decompression
• Instability following decompression• Deformity such as degenrative scoliosis or
kyphosis.
Fusion can be done in conjunction with decompression in …

Adjacent segment degeneration
• In 35%-45% patients post fusion• Due to hypermobility of unfused joint
usually above the fusion mass• Rigidity of instrumentation has been
thought to correlate with motion at adjacent segment
• Post operative hypolordosis have also been thought of as a cause.
Less invasive decompression procedures
• The consequences of bone and ligament removal must be considered when performing decompression for spinal stenosis.
• Removal of the spinous processes, laminae, variable portions of the facets and pars, supraspinous and interspinous ligaments, ligamentum flavum, and portions of facet capsules is routine during these operative procedures.
• Denervation of the paraspinal musculature occurs with wide exposures, which results in altered muscle function.
• A minimally invasive technique allows decompression of the significant compressing anatomy while preserving paraspinal muscles, the spinous processes, and intervening supraspinous and interspinous ligaments.
Less invasive decompression procedures
• Microdecompression• Multiple laminotomies• Expansive lumbar laminoplasty• Distraction laminoplasty• Decompression through a "port-hole" approach• Spinous process distraction devices
Multiple laminotomies
• For bilateral radicular symptoms, some authors prefer to do bilateral laminotomies as an alternative to laminectomy and preserving the midline structures .
• Bilateral laminotomy at two or three levels requires a longer operating time than total laminec tomy at an equal number of levels.
• Multiple laminotomies may be associated with fewer incidences of postoperative instability but is associated with higher incidence of neurologic sequelae.
• Multiple lamino tomies may be indicated for mild to moderate degen erative stenosis or degenerative spondylolisthesis.
• Total laminectomy is to be preferred for patients with severe degenerative stenosis or marked degenerative spondylolisthesis
Complications of surgery
• Intra operatively - Nerve root damage and dural lacerations
• CSF fistulas and pseudomeningocoeles
• Recurrent stenosis due to postoperative bone regrowth
• Postoperative facet or pars fracture
Complications of surgery
• Infection - could be superficial infection or deep infection.
• Deep infection includes discitis, epidural or transdural empyema leading to meningitis and adhesive arachnoiditis, osteomyelitis and para spinal abscess formation.
• Haemorrhage• Instability of the spine
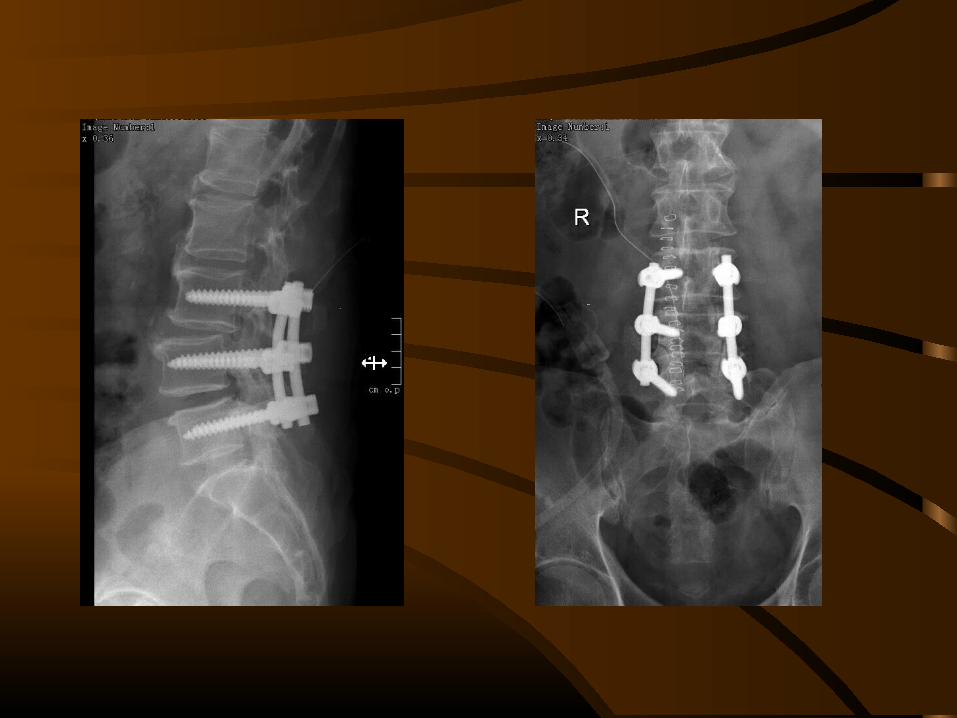
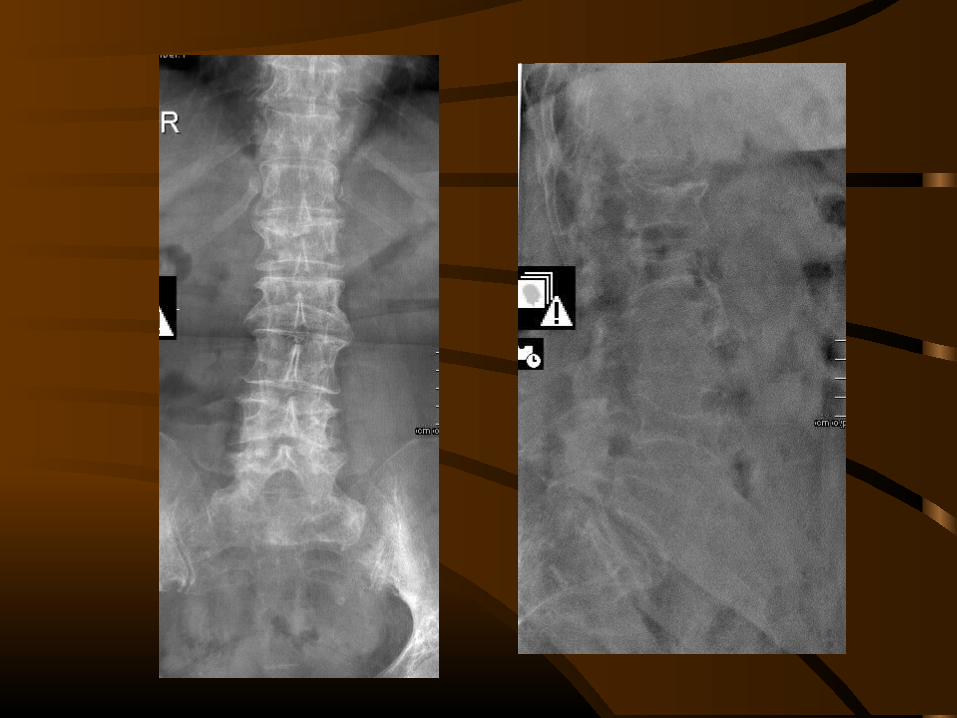
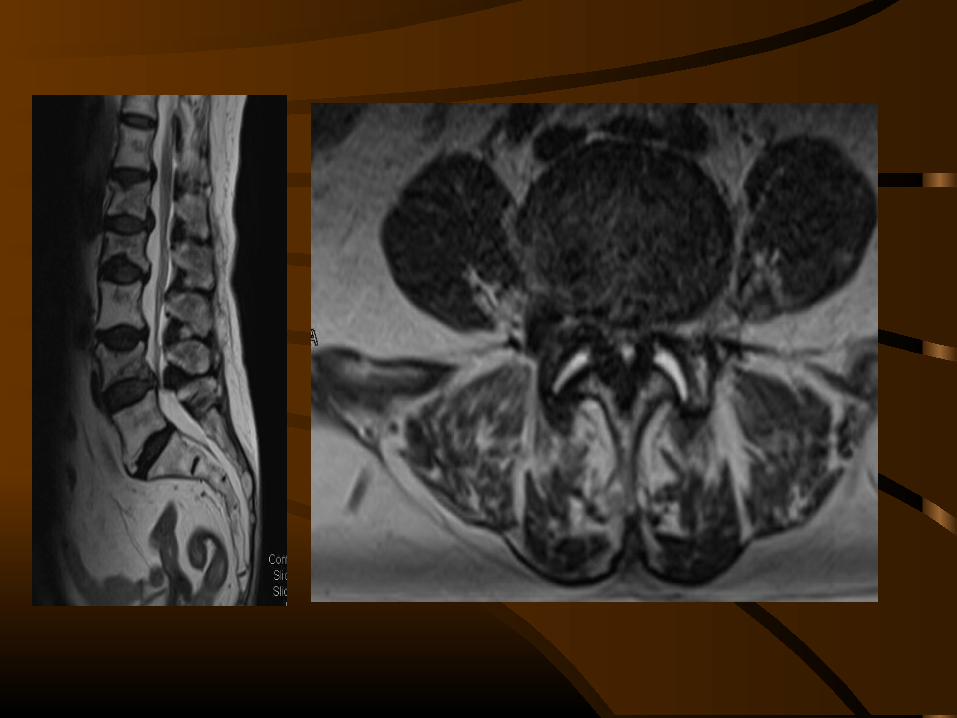
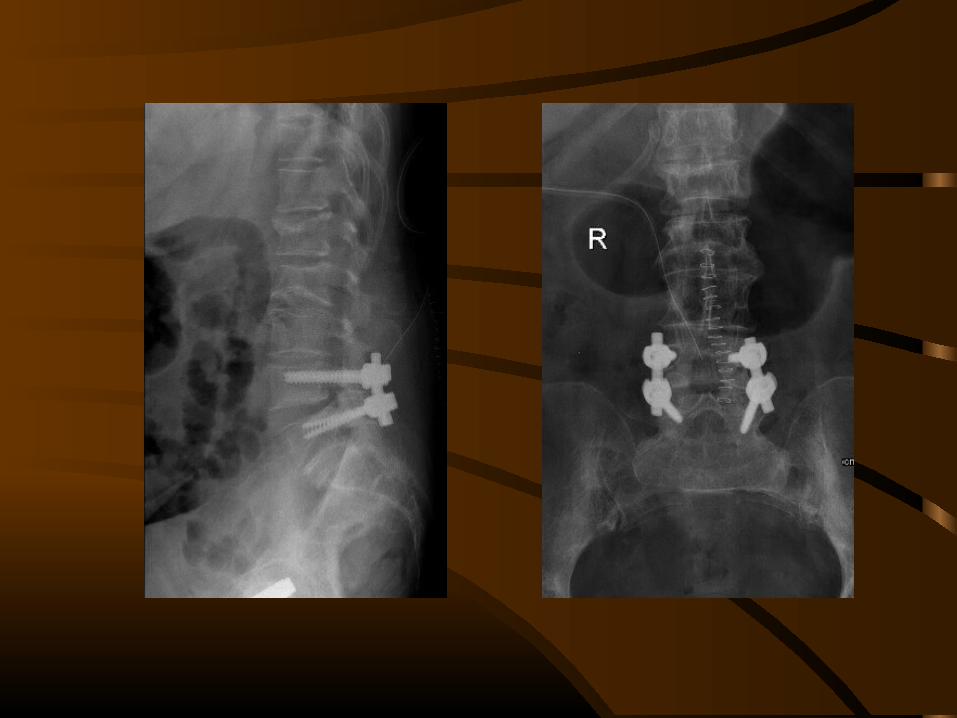
• 66/F• Symtoms – Backache and B/l legs pain
since 1 month with neurological deficit
Case 1:-
• 63/M• Sympoms- Backache and pain in right leg
since 5 years
Case 2:-