january 2018 page s disease -...
TRANSCRIPT
BU
LE
TIN
VOLUME 1/2018
JANUARY 2018
EDITORIAL BOARD ADVISOR: DR. SITI NORLINA BT. MD SAID EDITORS: PN SITI ROSNAH BT. SURADI PN NG WANG SING PN PATRICIA LIM MING HUA PN LI SHIN GIE
HOSPITAL SULTANAH AMINAH JOHOR BAHRU KEMENTERIAN KESIHATAN MALAYSIA JALAN PERSIARAN ABU BAKAR SULTAN 80100 JOHOR BAHRU TEL: 07-2257000 FAX: 07-2242694 EMAIL: [email protected]
IN THIS ISSUE ULCERATIVE COLITIS VS CROHN’S DISEASE
MANAGEMENT OF GOUT
MANAGEMENT OF SNAKEBITES
SUPPLEMENTATION IN PREGNANCY
PAGE 2 - 3
PAGE 4 - 5
PAGE 6 - 7
PAGE 8 - 9
MAJLIS PENGHARGAAN DR. SITI NORLINA BT MD SAID
PAGE 10
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 2
By: Pan Xue Hua
CROHN’S DISEASE (CD) ULCERATIVE COLITIS (UC)
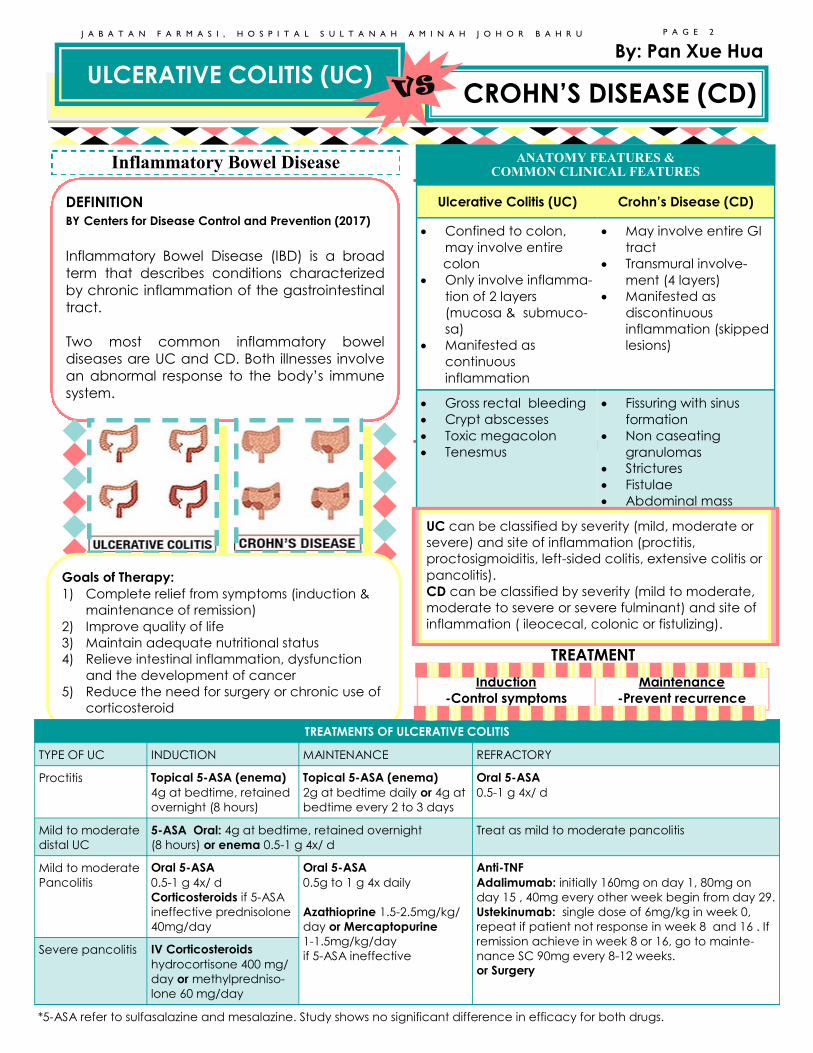
DEFINITION
BY Centers for Disease Control and Prevention (2017)
Inflammatory Bowel Disease (IBD) is a broad
term that describes conditions characterized
by chronic inflammation of the gastrointestinal
tract.
Two most common inflammatory bowel
diseases are UC and CD. Both illnesses involve
an abnormal response to the body’s immune
system.
Inflammatory Bowel Disease
ANATOMY FEATURES & COMMON CLINICAL FEATURES
Ulcerative Colitis (UC) Crohn’s Disease (CD)
• Confined to colon,
may involve entire
colon
• Only involve inflamma-
tion of 2 layers
(mucosa & submuco-
sa)
• Manifested as
continuous
inflammation
• May involve entire GI
tract
• Transmural involve-
ment (4 layers)
• Manifested as
discontinuous
inflammation (skipped
lesions)
• Gross rectal bleeding
• Crypt abscesses
• Toxic megacolon
• Tenesmus
• Fissuring with sinus
formation
• Non caseating
granulomas
• Strictures
• Fistulae
• Abdominal mass
UC can be classified by severity (mild, moderate or
severe) and site of inflammation (proctitis,
proctosigmoiditis, left-sided colitis, extensive colitis or
pancolitis).
CD can be classified by severity (mild to moderate,
moderate to severe or severe fulminant) and site of
inflammation ( ileocecal, colonic or fistulizing).
TREATMENT
Goals of Therapy:
1) Complete relief from symptoms (induction &
maintenance of remission)
2) Improve quality of life
3) Maintain adequate nutritional status
4) Relieve intestinal inflammation, dysfunction
and the development of cancer
5) Reduce the need for surgery or chronic use of
corticosteroid
Induction
-Control symptoms
Maintenance
-Prevent recurrence
TREATMENTS OF ULCERATIVE COLITIS
TYPE OF UC INDUCTION MAINTENANCE REFRACTORY
Proctitis Topical 5-ASA (enema)
4g at bedtime, retained
overnight (8 hours)
Topical 5-ASA (enema)
2g at bedtime daily or 4g at
bedtime every 2 to 3 days
Oral 5-ASA
0.5-1 g 4x/ d
Mild to moderate
distal UC
5-ASA Oral: 4g at bedtime, retained overnight
(8 hours) or enema 0.5-1 g 4x/ d
Treat as mild to moderate pancolitis
Mild to moderate
Pancolitis
Oral 5-ASA
0.5-1 g 4x/ d
Corticosteroids if 5-ASA
ineffective prednisolone
40mg/day
Oral 5-ASA
0.5g to 1 g 4x daily
Azathioprine 1.5-2.5mg/kg/
day or Mercaptopurine
1-1.5mg/kg/day
if 5-ASA ineffective
Anti-TNF
Adalimumab: initially 160mg on day 1, 80mg on
day 15 , 40mg every other week begin from day 29.
Ustekinumab: single dose of 6mg/kg in week 0,
repeat if patient not response in week 8 and 16 . If
remission achieve in week 8 or 16, go to mainte-
nance SC 90mg every 8-12 weeks.
or Surgery
Severe pancolitis IV Corticosteroids
hydrocortisone 400 mg/
day or methylpredniso-
lone 60 mg/day
*5-ASA refer to sulfasalazine and mesalazine. Study shows no significant difference in efficacy for both drugs.
REFERENCES:
1. Guidelines for the management of inflammatory bowel
disease in adults, 2011
2. Drug information handbook 24th edition
3. Applied Therapeutics: The Clinical Use of Drugs 10th edi-
tion.
4. A Study to Evaluate the Safety and Efficacy of Usteki-
numab Induction and Maintenance Therapy in Participants
With Moderately to Severely Active Ulcerative Colitis (UNIFI)
5. Simon, E. G., Ghosh, S., Iacucci, M., & Moran, G. W. (2016).
Ustekinumab for the treatment of Crohn’s disease: can it
find its niche? Therapeutic Advances in Gastroenterology,
9, 26–36. doi:10.1177/1756283X15618130
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 3
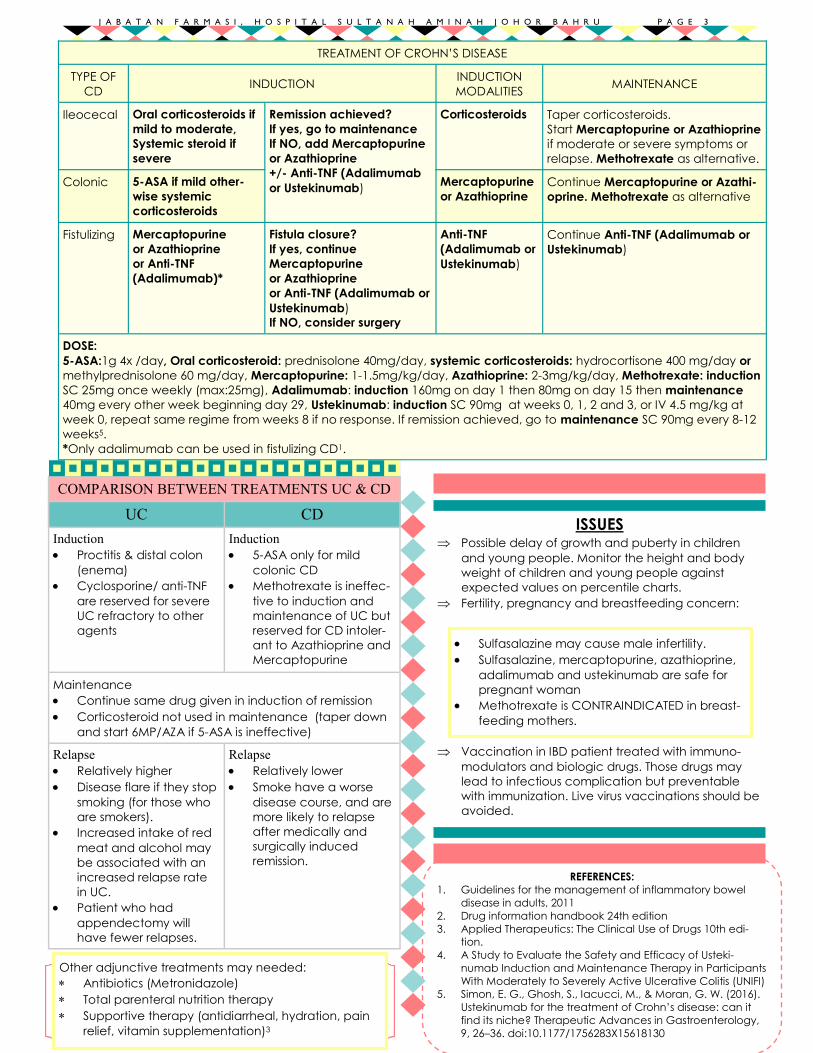
TREATMENT OF CROHN’S DISEASE
TYPE OF
CD INDUCTION
INDUCTION
MODALITIES MAINTENANCE
Ileocecal Oral corticosteroids if
mild to moderate,
Systemic steroid if
severe
Remission achieved?
If yes, go to maintenance
If NO, add Mercaptopurine
or Azathioprine
+/- Anti-TNF (Adalimumab
or Ustekinumab)
Corticosteroids Taper corticosteroids.
Start Mercaptopurine or Azathioprine
if moderate or severe symptoms or
relapse. Methotrexate as alternative.
Colonic 5-ASA if mild other-
wise systemic
corticosteroids
Mercaptopurine
or Azathioprine
Continue Mercaptopurine or Azathi-
oprine. Methotrexate as alternative
Fistulizing Mercaptopurine
or Azathioprine
or Anti-TNF
(Adalimumab)*
Fistula closure?
If yes, continue
Mercaptopurine
or Azathioprine
or Anti-TNF (Adalimumab or
Ustekinumab)
If NO, consider surgery
Anti-TNF
(Adalimumab or
Ustekinumab)
Continue Anti-TNF (Adalimumab or
Ustekinumab)
DOSE:
5-ASA:1g 4x /day, Oral corticosteroid: prednisolone 40mg/day, systemic corticosteroids: hydrocortisone 400 mg/day or
methylprednisolone 60 mg/day, Mercaptopurine: 1-1.5mg/kg/day, Azathioprine: 2-3mg/kg/day, Methotrexate: induction
SC 25mg once weekly (max:25mg), Adalimumab: induction 160mg on day 1 then 80mg on day 15 then maintenance
40mg every other week beginning day 29, Ustekinumab: induction SC 90mg at weeks 0, 1, 2 and 3, or IV 4.5 mg/kg at
week 0, repeat same regime from weeks 8 if no response. If remission achieved, go to maintenance SC 90mg every 8-12
weeks5.
*Only adalimumab can be used in fistulizing CD1.
COMPARISON BETWEEN TREATMENTS UC & CD
UC CD
Induction
• Proctitis & distal colon
(enema)
• Cyclosporine/ anti-TNF
are reserved for severe
UC refractory to other
agents
Induction
• 5-ASA only for mild
colonic CD
• Methotrexate is ineffec-
tive to induction and
maintenance of UC but
reserved for CD intoler-
ant to Azathioprine and
Mercaptopurine
Maintenance
• Continue same drug given in induction of remission
• Corticosteroid not used in maintenance (taper down
and start 6MP/AZA if 5-ASA is ineffective)
Relapse
• Relatively higher
• Disease flare if they stop
smoking (for those who
are smokers).
• Increased intake of red
meat and alcohol may
be associated with an
increased relapse rate
in UC.
• Patient who had
appendectomy will
have fewer relapses.
Relapse
• Relatively lower
• Smoke have a worse
disease course, and are
more likely to relapse
after medically and
surgically induced
remission.
Other adjunctive treatments may needed:
Antibiotics (Metronidazole)
Total parenteral nutrition therapy
Supportive therapy (antidiarrheal, hydration, pain
relief, vitamin supplementation)3
ISSUES Possible delay of growth and puberty in children
and young people. Monitor the height and body
weight of children and young people against
expected values on percentile charts.
Fertility, pregnancy and breastfeeding concern:
Vaccination in IBD patient treated with immuno-
modulators and biologic drugs. Those drugs may
lead to infectious complication but preventable
with immunization. Live virus vaccinations should be
avoided.
• Sulfasalazine may cause male infertility.
• Sulfasalazine, mercaptopurine, azathioprine,
adalimumab and ustekinumab are safe for
pregnant woman
• Methotrexate is CONTRAINDICATED in breast-
feeding mothers.
References
1. Janssens HJ et al. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. - PubMed - NCBI [Internet]. Ncbi.nlm.nih.gov. 2017 [cited 1 November 2017]. Available from: https://www.ncbi.nlm.nih.gov/pubmed?term=18514729
2. Prevention of recurrent gout: Pharmacologic urate-lowering therapy and treatment of tophi [Internet]. Uptodate.com. 2017 [cited 5 November 2017]. Avail-able from: www.uptodate.com/contents/prevention-of-recurrent-gout-pharmacologic-urate-lowering-therapy-and-treatment-of-tophi?source=history_widget
3. Clinical manifestations and diagnosis of gout [Internet]. Uptodate.com. 2017 [cited 5 November 2017]. Available from: https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-gout?source=search_result&search=gout&selectedTitle=2~150#H4
4. Clinical Practice Guidelines Malaysia. Management of Gout. 2008.
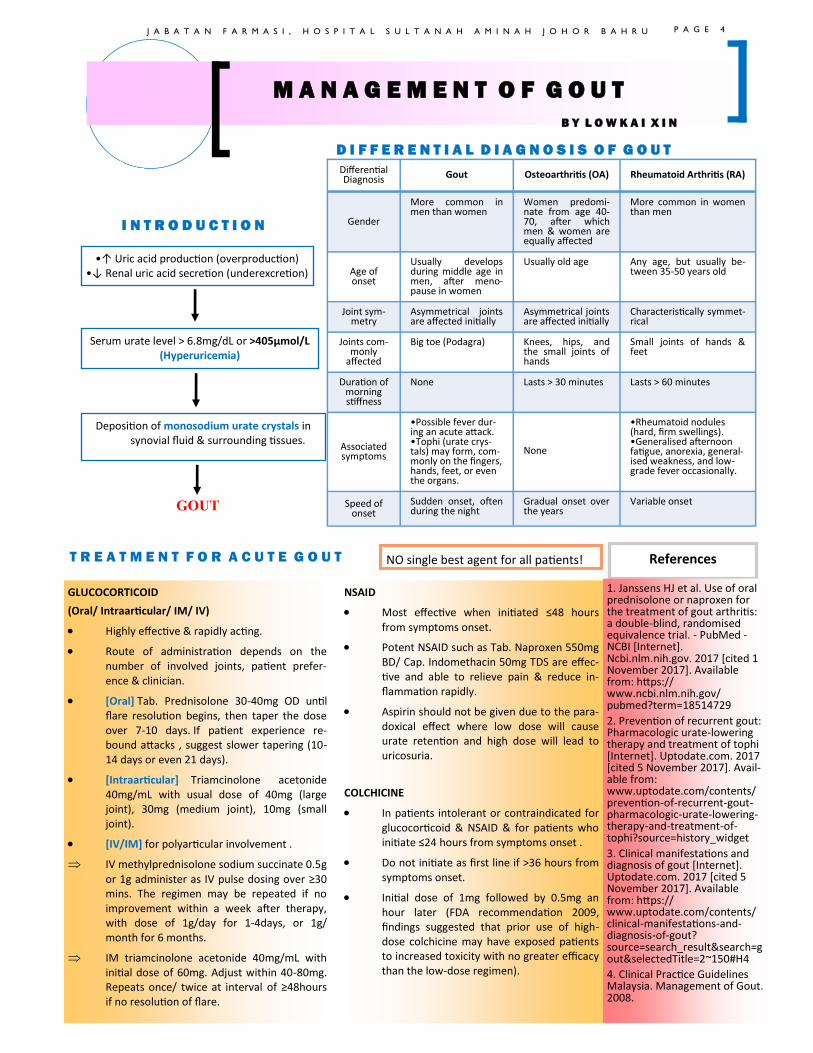
T R E A T M E N T F O R A C U T E G O U T
GLUCOCORTICOID
(Oral/ Intraarticular/ IM/ IV)
• Highly effective & rapidly acting.
• Route of administration depends on the number of involved joints, patient prefer-ence & clinician.
• [Oral] Tab. Prednisolone 30-40mg OD until flare resolution begins, then taper the dose over 7-10 days. If patient experience re-bound attacks , suggest slower tapering (10-14 days or even 21 days).
• [Intraarticular] Triamcinolone acetonide 40mg/mL with usual dose of 40mg (large joint), 30mg (medium joint), 10mg (small joint).
• [IV/IM] for polyarticular involvement .
IV methylprednisolone sodium succinate 0.5g or 1g administer as IV pulse dosing over ≥30 mins. The regimen may be repeated if no improvement within a week after therapy, with dose of 1g/day for 1-4days, or 1g/month for 6 months.
IM triamcinolone acetonide 40mg/mL with initial dose of 60mg. Adjust within 40-80mg. Repeats once/ twice at interval of ≥48hours if no resolution of flare.
NSAID
• Most effective when initiated ≤48 hours from symptoms onset.
• Potent NSAID such as Tab. Naproxen 550mg BD/ Cap. Indomethacin 50mg TDS are effec-tive and able to relieve pain & reduce in-flammation rapidly.
• Aspirin should not be given due to the para-doxical effect where low dose will cause urate retention and high dose will lead to uricosuria.
COLCHICINE
• In patients intolerant or contraindicated for glucocorticoid & NSAID & for patients who initiate ≤24 hours from symptoms onset .
• Do not initiate as first line if >36 hours from symptoms onset.
• Initial dose of 1mg followed by 0.5mg an hour later (FDA recommendation 2009, findings suggested that prior use of high-dose colchicine may have exposed patients to increased toxicity with no greater efficacy than the low-dose regimen).
M A N A G E M E N T O F G O U T
B Y L O W K A I X I N
I N T R O D U C T I O N
NO single best agent for all patients!
D I F F E R E N T I A L D I A G N O S I S O F G O U T
•↑ Uric acid production (overproduction) •↓ Renal uric acid secretion (underexcretion)
Serum urate level > 6.8mg/dL or >405µmol/L (Hyperuricemia)
Deposition of monosodium urate crystals in synovial fluid & surrounding tissues.
GOUT
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U
Differential Diagnosis Gout Osteoarthritis (OA) Rheumatoid Arthritis (RA)
Gender
More common in men than women
Women predomi-nate from age 40-70, after which men & women are equally affected
More common in women than men
Age of onset
Usually develops during middle age in men, after meno-pause in women
Usually old age Any age, but usually be-tween 35-50 years old
Joint sym-metry
Asymmetrical joints are affected initially
Asymmetrical joints are affected initially
Characteristically symmet-rical
Joints com-monly
affected
Big toe (Podagra) Knees, hips, and the small joints of hands
Small joints of hands & feet
Duration of morning stiffness
None Lasts > 30 minutes Lasts > 60 minutes
Associated symptoms
•Possible fever dur-ing an acute attack. •Tophi (urate crys-tals) may form, com-monly on the fingers, hands, feet, or even the organs.
None
•Rheumatoid nodules (hard, firm swellings). •Generalised afternoon fatigue, anorexia, general-ised weakness, and low-grade fever occasionally.
Speed of onset
Sudden onset, often during the night
Gradual onset over the years
Variable onset
P A G E 4
L I F E S T Y L E M O D I F I C A T I O N / R I S K R E D U C T I O N
S E C O N D - L I N E P H A R M A C O T H E R A P Y
F I R S T - L I N E P H A R M A C O T H E R A P Y
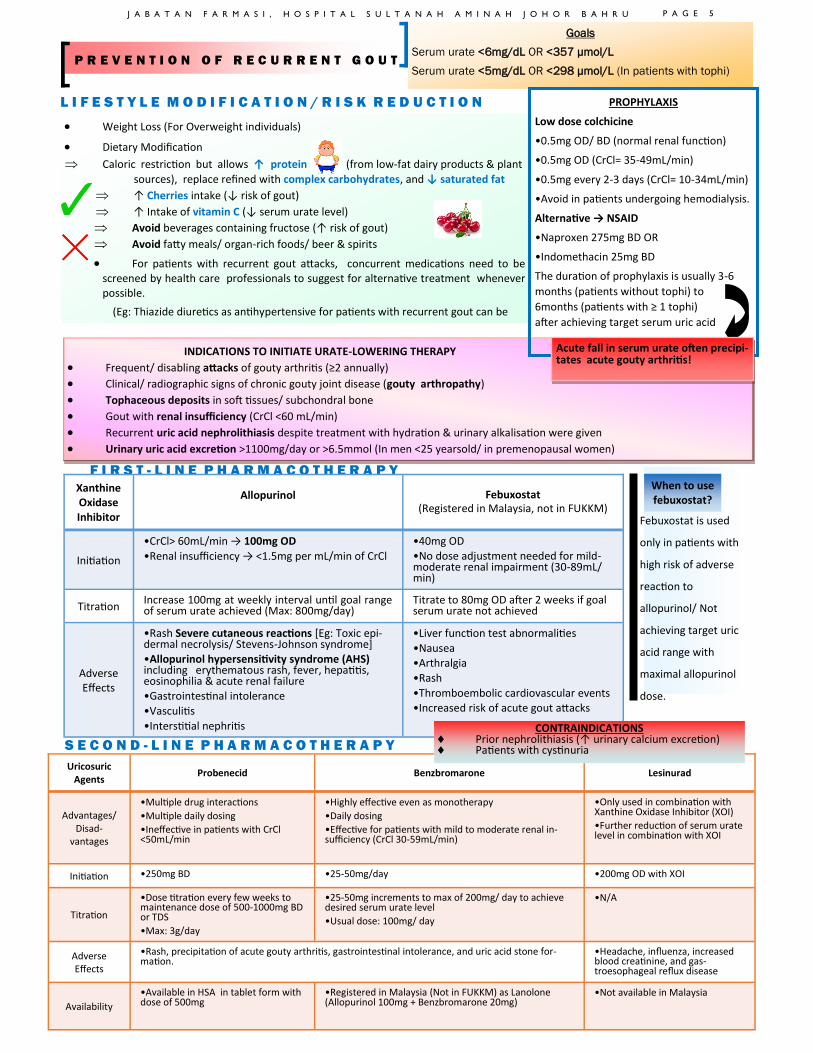
Febuxostat is used
only in patients with
high risk of adverse
reaction to
allopurinol/ Not
achieving target uric
acid range with
maximal allopurinol
dose.
P R E V E N T I O N O F R E C U R R E N T G O U T
• Weight Loss (For Overweight individuals)
• Dietary Modification
Caloric restriction but allows ↑ protein (from low-fat dairy products & plant
sources), replace refined with complex carbohydrates, and ↓ saturated fat
↑ Cherries intake (↓ risk of gout)
↑ Intake of vitamin C (↓ serum urate level)
Avoid beverages containing fructose (↑ risk of gout)
Avoid fatty meals/ organ-rich foods/ beer & spirits
• For patients with recurrent gout attacks, concurrent medications need to be screened by health care professionals to suggest for alternative treatment whenever possible.
(Eg: Thiazide diuretics as antihypertensive for patients with recurrent gout can be
Goals
Serum urate <6mg/dL OR <357 µmol/L
Serum urate <5mg/dL OR <298 µmol/L (In patients with tophi)
Uricosuric Agents
Probenecid Benzbromarone Lesinurad
Advantages/ Disad-
vantages
•Multiple drug interactions
•Multiple daily dosing
•Ineffective in patients with CrCl <50mL/min
•Highly effective even as monotherapy
•Daily dosing
•Effective for patients with mild to moderate renal in-sufficiency (CrCl 30-59mL/min)
•Only used in combination with Xanthine Oxidase Inhibitor (XOI)
•Further reduction of serum urate level in combination with XOI
Initiation •250mg BD •25-50mg/day •200mg OD with XOI
Titration
•Dose titration every few weeks to maintenance dose of 500-1000mg BD or TDS
•Max: 3g/day
•25-50mg increments to max of 200mg/ day to achieve desired serum urate level
•Usual dose: 100mg/ day
•N/A
Adverse Effects
•Headache, influenza, increased blood creatinine, and gas-troesophageal reflux disease
•Rash, precipitation of acute gouty arthritis, gastrointestinal intolerance, and uric acid stone for-mation.
Availability
•Available in HSA in tablet form with dose of 500mg
•Registered in Malaysia (Not in FUKKM) as Lanolone (Allopurinol 100mg + Benzbromarone 20mg)
•Not available in Malaysia
Xanthine Oxidase Inhibitor
Allopurinol
Febuxostat (Registered in Malaysia, not in FUKKM)
Initiation
•CrCl> 60mL/min → 100mg OD
•Renal insufficiency → <1.5mg per mL/min of CrCl
•40mg OD •No dose adjustment needed for mild- moderate renal impairment (30-89mL/min)
Titration Increase 100mg at weekly interval until goal range of serum urate achieved (Max: 800mg/day)
Titrate to 80mg OD after 2 weeks if goal serum urate not achieved
Adverse Effects
•Rash Severe cutaneous reactions [Eg: Toxic epi-dermal necrolysis/ Stevens-Johnson syndrome] •Allopurinol hypersensitivity syndrome (AHS) including erythematous rash, fever, hepatitis, eosinophilia & acute renal failure •Gastrointestinal intolerance
•Vasculitis
•Interstitial nephritis
•Liver function test abnormalities
•Nausea •Arthralgia
•Rash
•Thromboembolic cardiovascular events •Increased risk of acute gout attacks
CONTRAINDICATIONS Prior nephrolithiasis (↑ urinary calcium excretion) Patients with cystinuria
INDICATIONS TO INITIATE URATE-LOWERING THERAPY
• Frequent/ disabling attacks of gouty arthritis (≥2 annually)
• Clinical/ radiographic signs of chronic gouty joint disease (gouty arthropathy)
• Tophaceous deposits in soft tissues/ subchondral bone
• Gout with renal insufficiency (CrCl <60 mL/min)
• Recurrent uric acid nephrolithiasis despite treatment with hydration & urinary alkalisation were given
• Urinary uric acid excretion >1100mg/day or >6.5mmol (In men <25 yearsold/ in premenopausal women)
PROPHYLAXIS
Low dose colchicine
•0.5mg OD/ BD (normal renal function)
•0.5mg OD (CrCl= 35-49mL/min)
•0.5mg every 2-3 days (CrCl= 10-34mL/min)
•Avoid in patients undergoing hemodialysis.
Alternative → NSAID
•Naproxen 275mg BD OR
•Indomethacin 25mg BD
The duration of prophylaxis is usually 3-6
months (patients without tophi) to
6months (patients with ≥ 1 tophi)
after achieving target serum uric acid
Acute fall in serum urate often precipi-tates acute gouty arthritis!
When to use febuxostat?
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 5
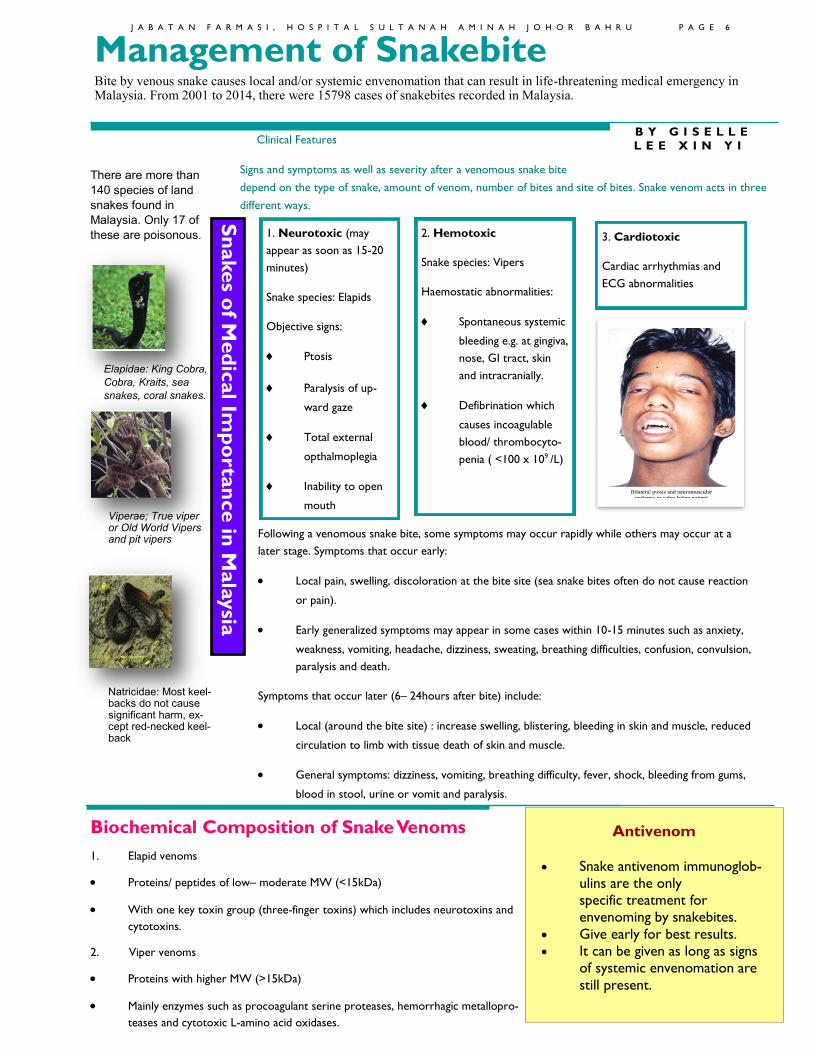
1. Neurotoxic (may
appear as soon as 15-20
minutes)
Snake species: Elapids
Objective signs:
Ptosis
Paralysis of up-
ward gaze
Total external
opthalmoplegia
Inability to open
mouth
Clinical Features
Signs and symptoms as well as severity after a venomous snake bite
depend on the type of snake, amount of venom, number of bites and site of bites. Snake venom acts in three
different ways.
Following a venomous snake bite, some symptoms may occur rapidly while others may occur at a
later stage. Symptoms that occur early:
• Local pain, swelling, discoloration at the bite site (sea snake bites often do not cause reaction
or pain).
• Early generalized symptoms may appear in some cases within 10-15 minutes such as anxiety,
weakness, vomiting, headache, dizziness, sweating, breathing difficulties, confusion, convulsion,
paralysis and death.
Symptoms that occur later (6– 24hours after bite) include:
• Local (around the bite site) : increase swelling, blistering, bleeding in skin and muscle, reduced
circulation to limb with tissue death of skin and muscle.
• General symptoms: dizziness, vomiting, breathing difficulty, fever, shock, bleeding from gums,
blood in stool, urine or vomit and paralysis.
B Y G I S E L L E
L E E X I N Y I
Management of Snakebite Bite by venous snake causes local and/or systemic envenomation that can result in life-threatening medical emergency in Malaysia. From 2001 to 2014, there were 15798 cases of snakebites recorded in Malaysia.
There are more than
140 species of land
snakes found in
Malaysia. Only 17 of
these are poisonous. 2. Hemotoxic
Snake species: Vipers
Haemostatic abnormalities:
Spontaneous systemic
bleeding e.g. at gingiva,
nose, GI tract, skin
and intracranially.
Defibrination which
causes incoagulable
blood/ thrombocyto-
penia ( <100 x 109 /L)
3. Cardiotoxic
Cardiac arrhythmias and
ECG abnormalities
Sn
akes o
f Med
ical Im
po
rta
nce in
Mala
ysia
Elapidae: King Cobra,
Cobra, Kraits, sea
snakes, coral snakes.
Viperae; True viper or Old World Vipers and pit vipers
Natricidae: Most keel-backs do not cause significant harm, ex-cept red-necked keel-back
Biochemical Composition of Snake Venoms
1. Elapid venoms
• Proteins/ peptides of low– moderate MW (<15kDa)
• With one key toxin group (three-finger toxins) which includes neurotoxins and
cytotoxins.
2. Viper venoms
• Proteins with higher MW (>15kDa)
• Mainly enzymes such as procoagulant serine proteases, hemorrhagic metallopro-
teases and cytotoxic L-amino acid oxidases.
Antivenom
• Snake antivenom immunoglob-
ulins are the only
specific treatment for
envenoming by snakebites.
• Give early for best results.
• It can be given as long as signs
of systemic envenomation are
still present.
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 6
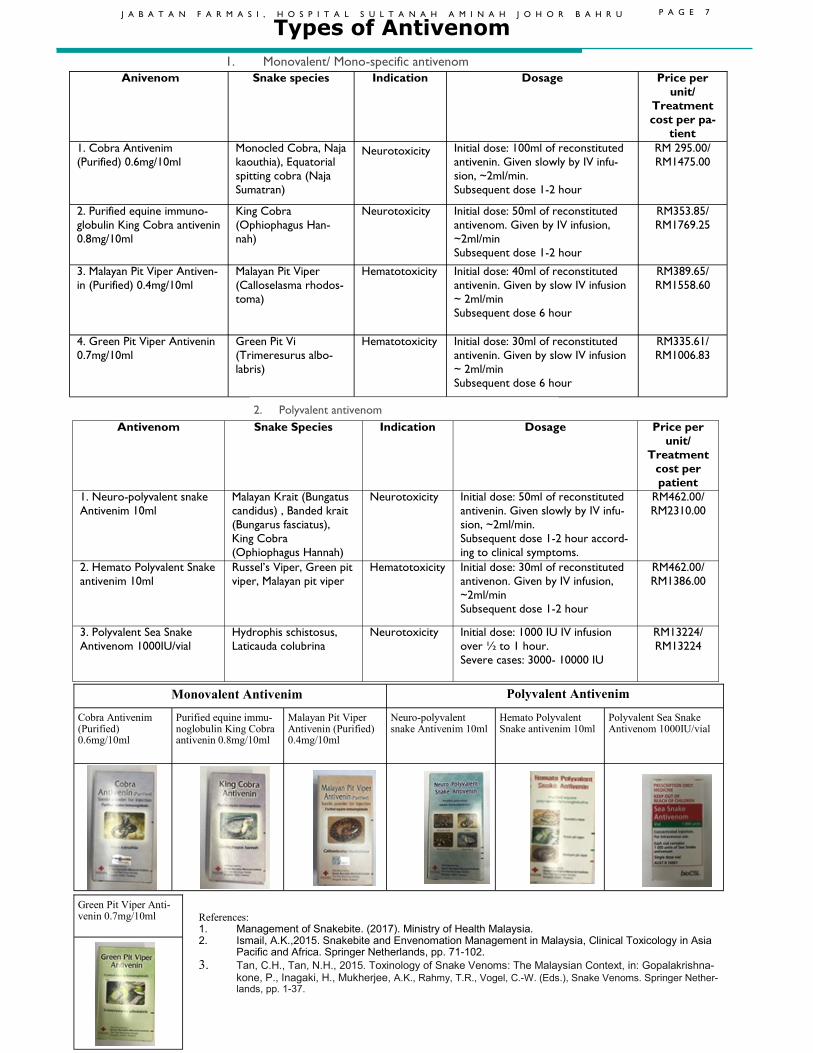
1. Monovalent/ Mono-specific antivenom
Types of Antivenom
Antivenom Snake Species Dosage Price per
unit/
Treatment
cost per
patient
Indication
1. Neuro-polyvalent snake
Antivenim 10ml
Malayan Krait (Bungatus
candidus) , Banded krait
(Bungarus fasciatus),
King Cobra
(Ophiophagus Hannah)
Initial dose: 50ml of reconstituted
antivenin. Given slowly by IV infu-
sion, ~2ml/min.
Subsequent dose 1-2 hour accord-
ing to clinical symptoms.
RM462.00/
RM2310.00
Neurotoxicity
2. Hemato Polyvalent Snake
antivenim 10ml
Russel’s Viper, Green pit
viper, Malayan pit viper
Initial dose: 30ml of reconstituted
antivenon. Given by IV infusion,
~2ml/min
Subsequent dose 1-2 hour
RM462.00/
RM1386.00
Hematotoxicity
3. Polyvalent Sea Snake
Antivenom 1000IU/vial
Hydrophis schistosus,
Laticauda colubrina
Initial dose: 1000 IU IV infusion
over ½ to 1 hour.
Severe cases: 3000- 10000 IU
RM13224/
RM13224
Neurotoxicity
Anivenom Snake species Dosage Price per
unit/
Treatment
cost per pa-
tient
Indication
1. Cobra Antivenim
(Purified) 0.6mg/10ml
Monocled Cobra, Naja
kaouthia), Equatorial
spitting cobra (Naja
Sumatran)
Initial dose: 100ml of reconstituted
antivenin. Given slowly by IV infu-
sion, ~2ml/min.
Subsequent dose 1-2 hour
RM 295.00/
RM1475.00 Neurotoxicity
2. Purified equine immuno-
globulin King Cobra antivenin
0.8mg/10ml
King Cobra
(Ophiophagus Han-
nah)
Initial dose: 50ml of reconstituted
antivenom. Given by IV infusion,
~2ml/min
Subsequent dose 1-2 hour
RM353.85/
RM1769.25
Neurotoxicity
3. Malayan Pit Viper Antiven-
in (Purified) 0.4mg/10ml
Malayan Pit Viper
(Calloselasma rhodos-
toma)
Initial dose: 40ml of reconstituted
antivenin. Given by slow IV infusion
~ 2ml/min
Subsequent dose 6 hour
RM389.65/
RM1558.60
Hematotoxicity
4. Green Pit Viper Antivenin
0.7mg/10ml
Green Pit Vi
(Trimeresurus albo-
labris)
Initial dose: 30ml of reconstituted
antivenin. Given by slow IV infusion
~ 2ml/min
Subsequent dose 6 hour
RM335.61/
RM1006.83
Hematotoxicity
2. Polyvalent antivenom
References: 1. Management of Snakebite. (2017). Ministry of Health Malaysia. 2. Ismail, A.K.,2015. Snakebite and Envenomation Management in Malaysia, Clinical Toxicology in Asia
Pacific and Africa. Springer Netherlands, pp. 71-102.
3. Tan, C.H., Tan, N.H., 2015. Toxinology of Snake Venoms: The Malaysian Context, in: Gopalakrishna-kone, P., Inagaki, H., Mukherjee, A.K., Rahmy, T.R., Vogel, C.-W. (Eds.), Snake Venoms. Springer Nether-lands, pp. 1-37.
Cobra Antivenim (Purified) 0.6mg/10ml
Purified equine immu-noglobulin King Cobra antivenin 0.8mg/10ml
Malayan Pit Viper Antivenin (Purified) 0.4mg/10ml
Neuro-polyvalent snake Antivenim 10ml
Hemato Polyvalent Snake antivenim 10ml
Polyvalent Sea Snake Antivenom 1000IU/vial
Monovalent Antivenim Polyvalent Antivenim
Green Pit Viper Anti-venin 0.7mg/10ml
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 7
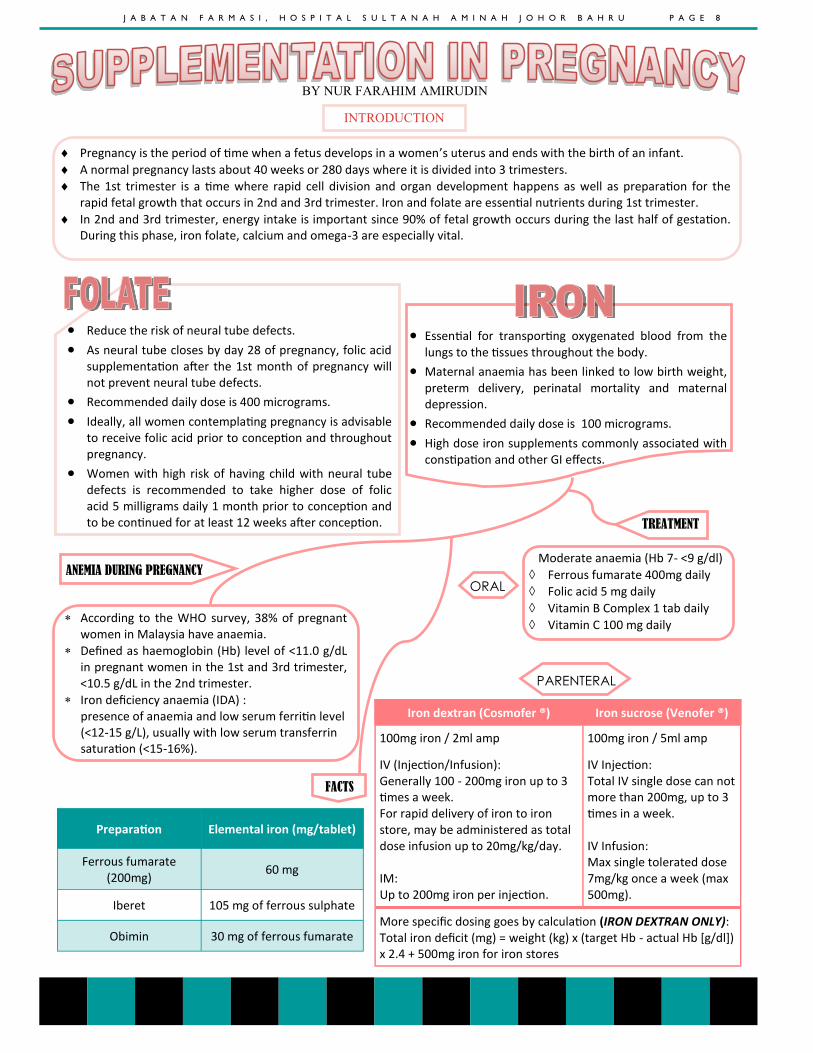
BY NUR FARAHIM AMIRUDIN
INTRODUCTION
Pregnancy is the period of time when a fetus develops in a women’s uterus and ends with the birth of an infant.
A normal pregnancy lasts about 40 weeks or 280 days where it is divided into 3 trimesters.
The 1st trimester is a time where rapid cell division and organ development happens as well as preparation for the rapid fetal growth that occurs in 2nd and 3rd trimester. Iron and folate are essential nutrients during 1st trimester.
In 2nd and 3rd trimester, energy intake is important since 90% of fetal growth occurs during the last half of gestation. During this phase, iron folate, calcium and omega-3 are especially vital.
• Reduce the risk of neural tube defects.
• As neural tube closes by day 28 of pregnancy, folic acid supplementation after the 1st month of pregnancy will not prevent neural tube defects.
• Recommended daily dose is 400 micrograms.
• Ideally, all women contemplating pregnancy is advisable to receive folic acid prior to conception and throughout pregnancy.
• Women with high risk of having child with neural tube defects is recommended to take higher dose of folic acid 5 milligrams daily 1 month prior to conception and to be continued for at least 12 weeks after conception.
• Essential for transporting oxygenated blood from the lungs to the tissues throughout the body.
• Maternal anaemia has been linked to low birth weight, preterm delivery, perinatal mortality and maternal depression.
• Recommended daily dose is 100 micrograms.
• High dose iron supplements commonly associated with constipation and other GI effects.
According to the WHO survey, 38% of pregnant women in Malaysia have anaemia.
Defined as haemoglobin (Hb) level of <11.0 g/dL in pregnant women in the 1st and 3rd trimester, <10.5 g/dL in the 2nd trimester.
Iron deficiency anaemia (IDA) : presence of anaemia and low serum ferritin level (<12-15 g/L), usually with low serum transferrin saturation (<15-16%).
Moderate anaemia (Hb 7- <9 g/dl)
Ferrous fumarate 400mg daily
Folic acid 5 mg daily
Vitamin B Complex 1 tab daily
Vitamin C 100 mg daily
Preparation Elemental iron (mg/tablet)
Ferrous fumarate (200mg)
60 mg
Iberet 105 mg of ferrous sulphate
Obimin 30 mg of ferrous fumarate
Iron dextran (Cosmofer ®) Iron sucrose (Venofer ®)
100mg iron / 2ml amp 100mg iron / 5ml amp
IV (Injection/Infusion): Generally 100 - 200mg iron up to 3 times a week. For rapid delivery of iron to iron store, may be administered as total dose infusion up to 20mg/kg/day. IM: Up to 200mg iron per injection.
IV Injection: Total IV single dose can not more than 200mg, up to 3 times in a week. IV Infusion: Max single tolerated dose 7mg/kg once a week (max 500mg).
More specific dosing goes by calculation (IRON DEXTRAN ONLY): Total iron deficit (mg) = weight (kg) x (target Hb - actual Hb [g/dl]) x 2.4 + 500mg iron for iron stores
TREATMENT
ANEMIA DURING PREGNANCY
ORAL
PARENTERAL
FACTS
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 8
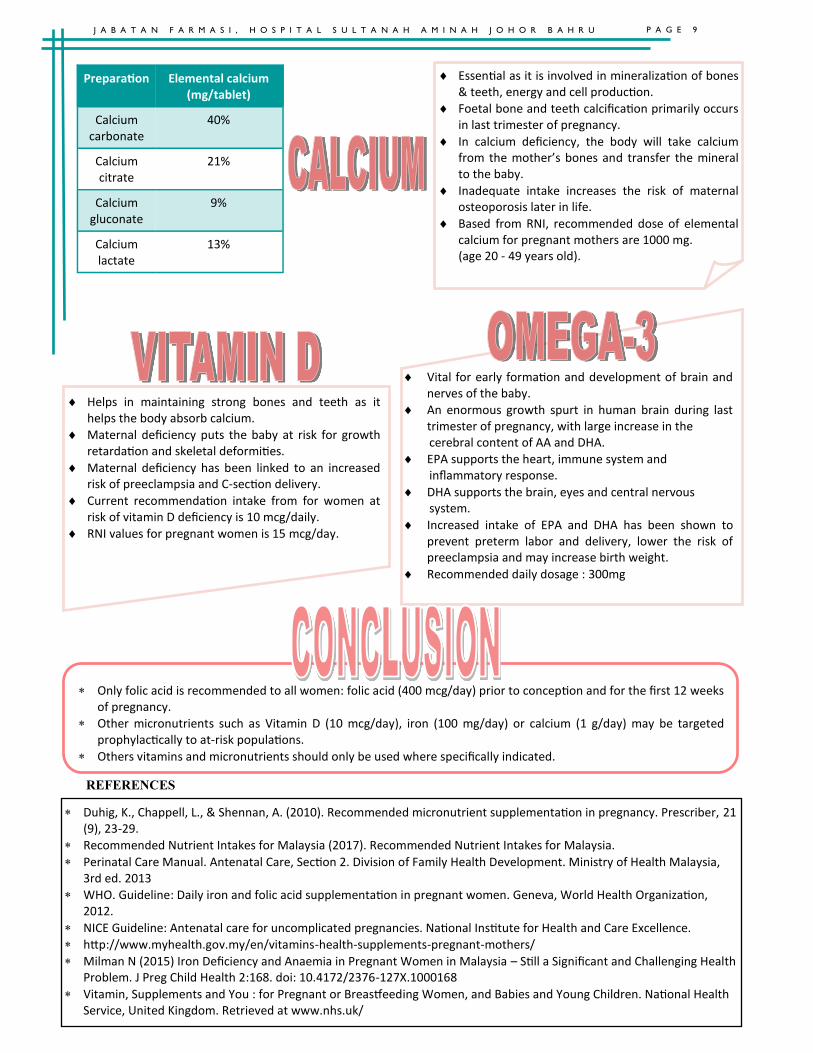
Helps in maintaining strong bones and teeth as it helps the body absorb calcium.
Maternal deficiency puts the baby at risk for growth retardation and skeletal deformities.
Maternal deficiency has been linked to an increased risk of preeclampsia and C-section delivery.
Current recommendation intake from for women at risk of vitamin D deficiency is 10 mcg/daily.
RNI values for pregnant women is 15 mcg/day.
Essential as it is involved in mineralization of bones & teeth, energy and cell production.
Foetal bone and teeth calcification primarily occurs in last trimester of pregnancy.
In calcium deficiency, the body will take calcium from the mother’s bones and transfer the mineral to the baby.
Inadequate intake increases the risk of maternal osteoporosis later in life.
Based from RNI, recommended dose of elemental calcium for pregnant mothers are 1000 mg.
(age 20 - 49 years old).
Preparation Elemental calcium (mg/tablet)
Calcium carbonate
40%
Calcium citrate
21%
Calcium gluconate
9%
Calcium lactate
13%
Vital for early formation and development of brain and nerves of the baby.
An enormous growth spurt in human brain during last trimester of pregnancy, with large increase in the
cerebral content of AA and DHA.
EPA supports the heart, immune system and inflammatory response.
DHA supports the brain, eyes and central nervous system.
Increased intake of EPA and DHA has been shown to prevent preterm labor and delivery, lower the risk of preeclampsia and may increase birth weight.
Recommended daily dosage : 300mg
Only folic acid is recommended to all women: folic acid (400 mcg/day) prior to conception and for the first 12 weeks of pregnancy.
Other micronutrients such as Vitamin D (10 mcg/day), iron (100 mg/day) or calcium (1 g/day) may be targeted prophylactically to at-risk populations.
Others vitamins and micronutrients should only be used where specifically indicated.
Duhig, K., Chappell, L., & Shennan, A. (2010). Recommended micronutrient supplementation in pregnancy. Prescriber, 21(9), 23-29.
Recommended Nutrient Intakes for Malaysia (2017). Recommended Nutrient Intakes for Malaysia.
Perinatal Care Manual. Antenatal Care, Section 2. Division of Family Health Development. Ministry of Health Malaysia, 3rd ed. 2013
WHO. Guideline: Daily iron and folic acid supplementation in pregnant women. Geneva, World Health Organization, 2012.
NICE Guideline: Antenatal care for uncomplicated pregnancies. National Institute for Health and Care Excellence.
http://www.myhealth.gov.my/en/vitamins-health-supplements-pregnant-mothers/
Milman N (2015) Iron Deficiency and Anaemia in Pregnant Women in Malaysia – Still a Significant and Challenging Health Problem. J Preg Child Health 2:168. doi: 10.4172/2376-127X.1000168
Vitamin, Supplements and You : for Pregnant or Breastfeeding Women, and Babies and Young Children. National Health Service, United Kingdom. Retrieved at www.nhs.uk/
REFERENCES
P A G E 9 J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U
J A B A T A N F A R M A S I , H O S P I T A L S U L T A N A H A M I N A H J O H O R B A H R U P A G E 1 0
MAJLIS PENGHARGAAN
DR. SITI NORLINA BINTI MD SAID Oleh Jaswinder Kaur
Majlis Malam Sekalung Budi Ketua Pegawai Farmasi dan Masquerade Night 2018 Hospital Sultanah Aminah Johor Bahru (HSAJB) anjuran bersama Kelab Sukan dan Kebajikan Perubatan, Kesihatan dan Pergigian Johor Bahru telah diadakan pada 25hb Januari 2018 di KSL Hotel & Resort. Majlis ini merupakan majlis khusus yang diadakan sempena meraikan persaraan Dr. Siti Norlina binti Md Said sebagai Ketua Pegawai Farmasi. Majlis ini telah diadakan bagi mengenang jasa dan keringat yang telah dicurahkan oleh beliau selama berkhidmat di Jabatan Farmasi, HSAJB.
Majlis ini turut sama dihadiri oleh Dr. Aman bin Rabu (Pengarah HSAJB), Pn Sarinah binti Apisah (Timbalan Pengarah Pengurusan) dan Cik Suraya Hanim binti Sith (Penolong Pengarah Kanan). Para Pesara Jabatan Farmasi juga dijemput bagi memeriahkan majlis pada hari tersebut.
Majlis dimulakan dengan bacaan doa bagi memberkati majlis dan diteruskan dengan ucapan oleh tetamu jemputan. Majlis dimeriahkan dengan jamuan makan malam, acara potong kek, dan persembahan oleh Pegawai Farmasi, Pegawai Farmasi Provisional dan Penolong Pegawai Farmasi. Sebanyak 3 sesi cabutan bertuah dan acara permainan ringkas diadakan pada hari tersebut.
Majlis diteruskan dengan ucapan oleh Dr. Siti Norlina binti Md Said. Beliau mengambil kesempatan mengucapkan setinggi-tinggi penghargaan dan terima kasih kepada warga farmasi HSAJB yang selama ini banyak membantu dan memberi kerjasama kepada beliau. Majlis diteruskan dengan acara penyampaian hadiah kepada Dr. Siti Norlina binti Md Said.
Majlis diakhiri dengan penyampaian hadiah kepada pemenang “Best Dress”, sesi cabutan bertuah “Grand Price”dan sesi fotografi berkumpulan. Secara keseluruhan, majlis berjalan dengan lancar sepertimana yang telah dirancangkan.